PCI during an acute myocardial infarction is not the kind of case where coding should rest on assumption. It is urgent. The artery matters. The reason for treatment should be easy to see in the record. When an interventional cardiologist performs emergency PCI on the culprit vessel, CPT code 92941 should be reported.
This code is used for a more serious level of service. So payment is often higher than it is for many other coronary procedures. At the same time, payers may look at the chart more closely. To support CPT 92941, the record should clearly show the acute MI, the emergency nature of the procedure, and the vessel that caused the infarction.
What is CPT code 92941?
CPT code 92941 is used for urgent coronary treatment during a heart attack. It applies when an interventional cardiologist treats the blocked artery that caused the event and restores blood flow in one vessel.
Because this is an urgent case, the work may involve more than one step during the same procedure. For example, the interventional cardiologist may use a balloon to open the artery, place a stent to help keep it open, or remove a clot that is blocking blood flow. In some cases, atherectomy may also be needed. Along with that, the code includes the imaging used to see the artery and guide the treatment.
This code is most often used in STEMI cases. However, it may also apply in some emergent NSTEMI cases when the patient still has chest pain or ongoing low blood flow and needs urgent PCI.
What matters most, though, is which vessel is being treated. For CPT code 92941 to apply, the interventional cardiologist must treat the culprit vessel, meaning the artery responsible for the heart attack. Just as important, the code applies to one vessel only.
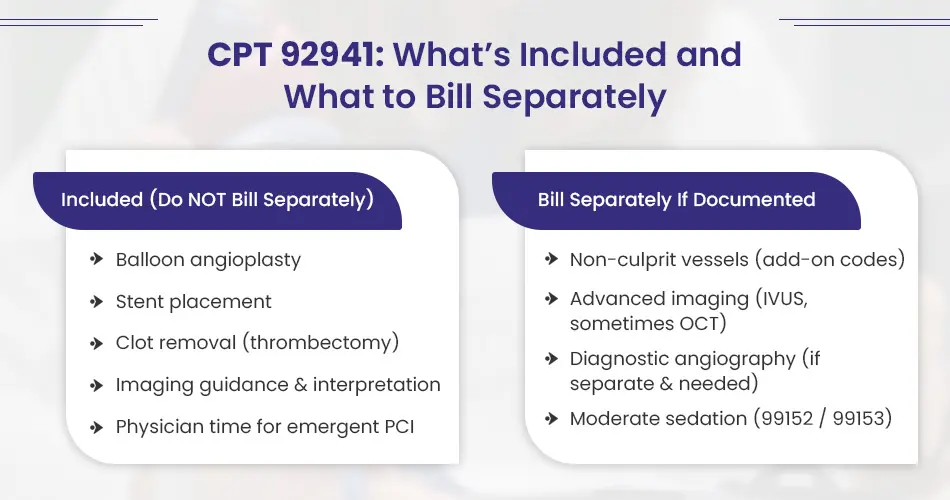
Services Included in CPT 92941
CPT 92941 already covers the main work done to treat the blocked artery during an acute myocardial infarction. Because of that, the services below are included in the code and should not be billed on their own:
- balloon angioplasty
- stent placement
- manual thrombectomy or clot removal
- imaging guidance and interpretation used during the procedure
- physician work tied to performing the emergency PCI
Put simply, CPT 92941 covers the work needed to open the blocked coronary artery during treatment of an acute MI. So, when those services are part of that same intervention, billing them one by one will lead to a claim denial.
Services Not Included in CPT 92941
Some services fall outside CPT 92941. When the record supports them, those services may be billed separately.
1. Work in non-culprit vessels
CPT 92941 applies to the culprit vessel only. So, if the interventional cardiologist also performs PCI in a non-culprit vessel, that work is not included in 92941.
Coding in this area has changed under the 2026 CPT updates. The branch or add-on codes 92921, 92925, 92929, and 92934 have been removed. As a result, coders now need to report the appropriate primary code for each procedure based on the vessels treated and the full details of the case, such as multi-vessel, multi-lesion, or bifurcation work.
Because of that shift, code choice should follow the most current CPT guidelines and the procedure note.
2. Advanced imaging
Some imaging is built into CPT 92941, but not all imaging falls under that umbrella. When the record shows clear clinical need, IVUS may be billed separately with 92978 and 92979.
In some cases, OCT may also be billed separately. That said, separate billing depends on clear documentation showing why the service was needed.
3. Diagnostic angiography
Diagnostic angiography is not automatically separate just because it appears in the same case. It may be billed separately only when it stands apart from the PCI work itself.
That usually means one of the following is true:
- no prior angiogram is available
- the patient’s clinical status changed and a new assessment was needed
- the diagnostic findings directly shaped the decision to perform PCI
If none of those conditions are met, separate billing would not apply.
4. Moderate sedation
Moderate sedation may also be billed separately when it is properly documented. The usual codes are:
- 99152 for the first 15 minutes
- 99153 for each additional 15 minutes
Documentation Required to Support 92941 Procedure Code
To support billing and coverage for 92941 CPT code, the record needs to clearly show why the procedure was medically necessary and what was done during the case. In many denials, the problem is not the procedure itself. The problem is that the documentation does not fully support the service billed.
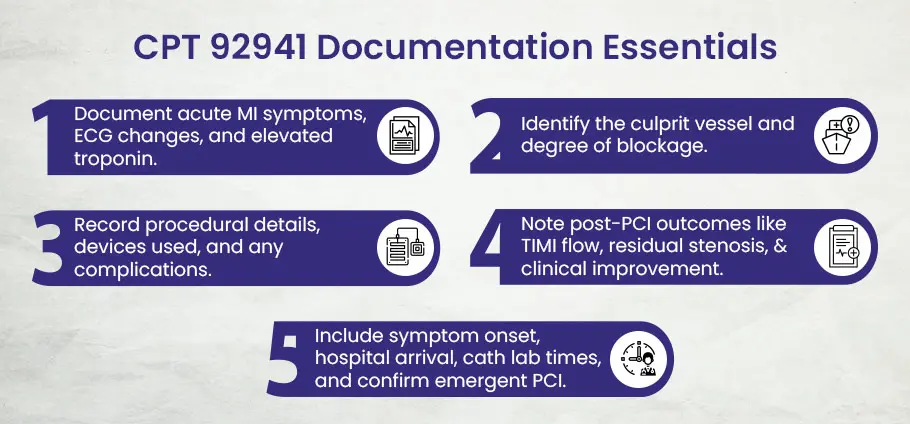
1). Proof of acute myocardial infarction
Start by showing that the patient was having an acute myocardial infarction. The note should describe the patient’s symptoms, such as chest pain, shortness of breath, diaphoresis, or syncope. It should also include ECG findings, such as new ST elevation, left bundle branch block, or other signs of ischemia.
Cardiac biomarkers should be part of the record as well. For example, elevated troponin or cardiac-specific troponin levels can help support the diagnosis. At the same time, the note should describe the patient’s hemodynamic status, including hypotension, cardiogenic shock, or any other sign of instability, if present.
Taken together, this part of the record helps show that the PCI was emergent and medically necessary, not planned or elective.
2). Angiography findings
The angiography report should clearly identify the culprit vessel that caused the myocardial infarction. This may be the LAD, RCA, or LCX, depending on the case. The report should also describe how severe the blockage was, including whether there was subtotal stenosis or full occlusion, such as 100 percent blockage.
Just as important, the documentation should note whether thrombus was present and should include the pre-PCI TIMI flow grade, such as TIMI 0 or TIMI 1.
This section matters because coronary intervention code 92941 applies only when the PCI is performed on the culprit vessel tied to the acute MI.
3). Technical details of the procedure
The procedure note should also explain how the intervention was performed. That includes the vessel treated and the vascular access site used. It should name the devices used during the case, such as the balloon, stent type and size, or atherectomy device when one is used.
The note should also capture the main technical details of the work itself. That may include balloon inflation pressure, the number of stents placed, lesion features, and any added techniques used during the case, such as thrombectomy or extra imaging.
If any complications occurred, those should be documented too. Examples include dissection, perforation, or arrhythmia.
All of this helps support the level of work performed and may also support any separately billable service when it is allowed and properly documented. Clear technical detail also gives your medical billing company stronger support when preparing or defending the claim.
4). Patient outcome after the procedure
The record should not stop once the procedure ends. It should also show the result of the intervention.
That means documenting the post-procedure TIMI flow grade, such as TIMI 3 for normal flow. It should also include the percent of residual stenosis, such as less than 10 percent, along with any clinical improvement seen after treatment. For example, the note may show relief of chest pain or improved perfusion.
These details help show the effect of the procedure and complete the clinical picture.
5). Urgency and timing
Because PCI code 92941 is tied to emergent care, the timeline matters. The record should include the time symptoms began, if known, along with the time the patient arrived at the hospital and the time the cardiac catheterization lab was activated.
It should also clearly state that the PCI was performed on an emergent basis due to an acute MI. If available, door-to-balloon time should be included as well.
A vague line such as “urgent attempt” is usually not enough on its own. Payers want clear written support showing that the PCI was truly emergent.
Does 92941 Procedure Code Need Prior Authorization?
Most of the time, no. CPT 92941 is used for an emergency PCI during a heart attack. Because of that, prior authorization is usually not required.
Medicare does not usually require prior authorization for this service. Medicare Advantage plans also often waive it. Still, they may review the chart later. That review helps them confirm that the case was truly urgent and medically needed.
The same is often true for commercial insurance. Medicaid also usually does not require prior authorization for an emergent PCI. However, some states may have different rules for an elective PCI.
The main point is clear. Prior authorization usually applies to elective PCI, not to CPT 92941 when the case is emergent.
2026 RVU Breakdown for CPT 92941
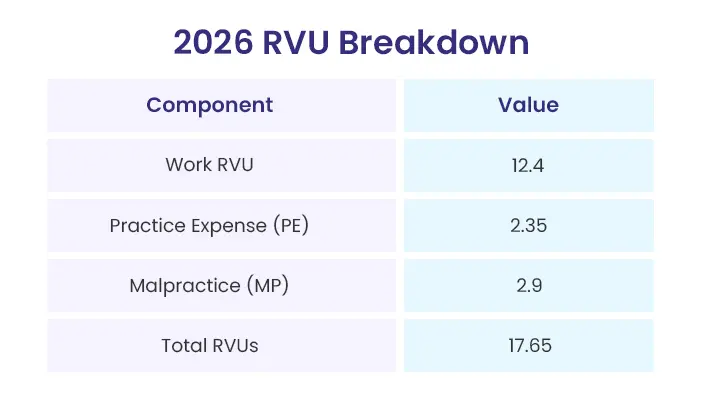
The RVU system helps show how physician pay is set for a service. For CPT 92941, the total for 2026 is 17.65 RVUs.
That total breaks down like this:
- Work RVUs: 12.4
- Practice Expense (PE) RVUs: 2.35
- Malpractice (MP) RVUs: 2.9
- Total RVUs: 17.65
Most of the RVU value comes from the physician’s work. In this case, about 70% of the total comes from the physician’s time, skill, and judgment during the emergency PCI.
The RVU values are also close in both office and facility settings. Because of that, physician payment can be figured in a more consistent way across care settings.
Physician Reimbursement Rates for 92941 CPT Code
| Component | Typical Payment | Notes |
|---|---|---|
| Physician (Medicare) | ~$625 | Based on total RVUs |
| Physician (Commercial) | $880–$1,070 | Varies by contract and region |
| Hospital (Medicare) | Several thousand | Covers staff, devices, and supplies |
Medicare Payment
For the physician side of 92941 procedure code, Medicare pays about $625 on a national average basis.
That number comes from the code’s total 17.65 RVUs and the Medicare conversion factor for the year. It is the professional fee only. It does not include what the hospital gets paid.
The number can shift a bit from one year to the next. Still, it gives a solid point of reference when you want a rough Medicare payment amount for the physician’s work.
Commercial Insurance Payment
Commercial plans usually pay more than Medicare for this kind of case. How much more depends on the contract and where the service is billed.
Typical estimates often look like this:
- BCBS: about $930
- UHC: about $920
- Aetna: about $880
- Cigna: about $1,070
So while there is no one fixed number across all plans, commercial payment often lands well above Medicare for a high-acuity case like an emergency PCI. In day-to-day medical billing for cardiology service, that difference can have a real effect on revenue expectations and claim planning.
Hospital Reimbursement
Hospital reimbursement sits apart from the physician fee. It is a separate payment, and in most cases, it is much higher. The reason is simple: the hospital payment covers far more than the professional work alone. It covers the use of the cardiac catheterization lab, along with staff time, supplies, drugs, and the devices used during the procedure, including balloons and stents.
From there, the payment method shifts based on the patient’s status. If the PCI is billed as outpatient, Medicare usually pays the hospital through OPPS. If the case is billed as inpatient, payment usually falls under IPPS.
Because of that, hospital payment is not tied to coronary intervention code 92941 by itself. Instead, Medicare places the case into a broader payment group. For outpatient cases, that means APCs. For inpatient cases, it means DRGs.
That is also why there is no single public hospital payment linked only to PCI billing code 92941.
As for what hospitals usually receive, there is no one flat amount that fits every case. The final number can move for several reasons. Even so, emergent PCI cases often bring in several thousand dollars on the hospital side under Medicare.
The amount can rise or fall based on whether the patient is inpatient or outpatient, the local wage index, device-related payment adjustments, and the type of hospital performing the case. So even when two procedures look much the same on paper, a small community hospital and a large academic center may not be paid the same way.
Most Common Reasons CPT Code 92941 Gets Denied And What Helps Prevent Those Denials
92941 procedure code is often denied when the medical record does not fully support the claim. In many cases, the central problem is that the chart does not clearly show that the patient had an acute myocardial infarction. The code may be billed for an acute MI, but if the record leaves too much unsaid, the claim becomes hard to defend infront of the payer.
Below are some of the denial issues that come up most often, along with what should appear in the record to support the code more clearly.
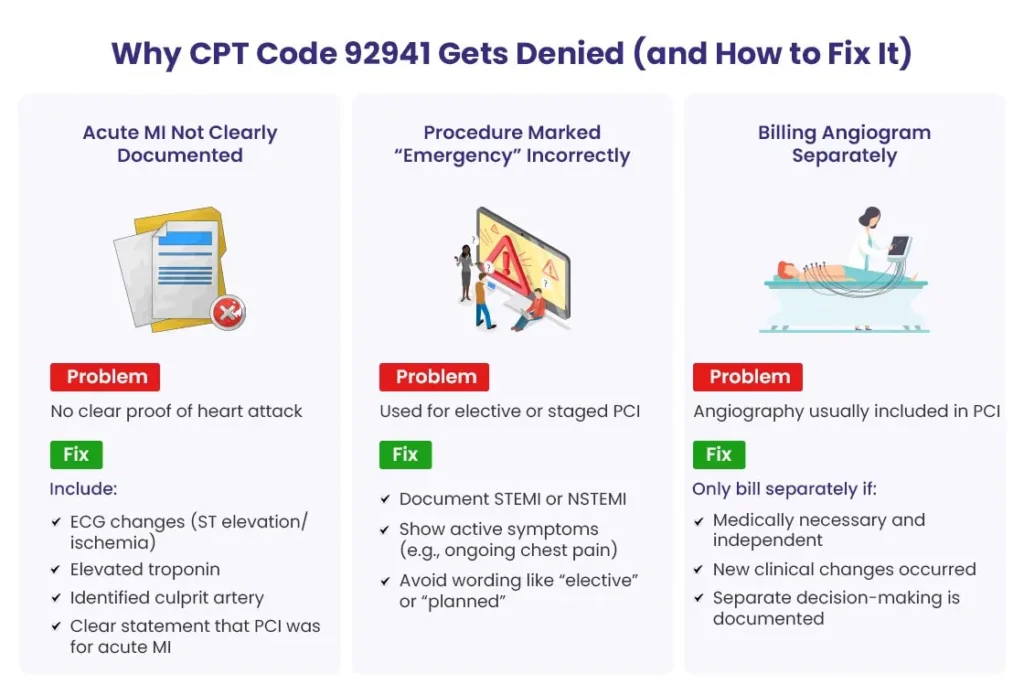
1). The acute myocardial infarction is not clearly documented
➜ Why it gets denied
92941 CPT code depends on proof that the patient was having an acute myocardial infarction. That point cannot be vague or implied. If the note mentions chest pain, possible ischemia, or concern for MI without clearly showing that an acute infarction occurred, payers may deny the claim.
The issue is not always that the care was wrong. Often, the issue is that the record never states the condition in a way that firmly supports the code.
➜ How to fix it
The documentation should clearly show the acute MI through findings that support the diagnosis. That may include:
- electrocardiogram findings that show ischemic change or ST elevation
- elevated cardiac biomarkers, such as troponin
- clear identification of the artery or lesion tied to the infarction
The record should also make it plain that the PCI was performed because of the acute myocardial infarction. A note that only mentions chest pain or suspected ischemia leaves too much open to interpretation.
2). The claim is billed as an emergency, but the record does not fully read that way
➜ Why it gets denied
PCI code 92941 is used for PCI performed in the setting of an acute MI. When the documentation sounds more like a planned case, a staged case, or treatment for stable coronary disease, the emergency nature of the claim becomes harder to support.
In some cases, the denial does not come from one sentence alone. It comes from the overall feel of the note. The claim presents the case as urgent, but the record does not carry that same sense of urgency from start to finish.
➜ How to fix it
The note should clearly name the diagnosis, such as STEMI or NSTEMI, and it should describe the patient’s presentation in a way that fits an active infarction.
That may include documentation of:
- acute chest pain
- ongoing ischemia
- active infarction
- urgent need for PCI
It also helps to avoid wording that makes the case sound elective, scheduled, or staged. Even when the right service was performed, the wrong tone in the record can create doubt.
3). Diagnostic angiography is billed separately without enough support
➜ Why it gets denied
Diagnostic coronary angiography is often part of the overall PCI case. Because of that, it is not always separately billable. When it is billed as a separate service, the record has to show why it stood apart from the intervention itself.
If that distinction is missing, the separate charge may be denied.
➜ How to fix it
Separate billing works best when the documentation shows that the diagnostic angiography had its own medical purpose and was not simply part of the PCI.
That usually means the record supports one of the following:
- the diagnostic angiography was medically necessary as a separate service
- no prior angiogram was available
- the patient’s condition changed enough to require a new diagnostic assessment
- the findings directly affected the decision to proceed with PCI
What matters most is not just that the angiography was performed. What matters is whether the record shows why it deserved to stand on its own.
ICD-10 Codes for Emergency Coronary Angioplasty (CPT 92941)
For CPT 92941 to be reported correctly, the record must show an acute myocardial infarction. That is the starting point. Without clear evidence of an acute MI, the claim is very likely to be denied.
In practical terms, this means the diagnosis code has to do more than describe symptoms or related heart problems. It has to show that the patient was being treated for an acute infarction.
Primary diagnosis codes to use first
When CPT 92941 is reported, the primary diagnosis should usually come from the I21 category, since that group reflects an acute myocardial infarction and helps support medical need for an emergency PCI.
The most common first-choice codes include:
- I21.01 – STEMI involving left main coronary artery
- I21.02 – STEMI involving the LAD (left anterior descending) artery
- I21.11 – STEMI involving right coronary artery
- I21.21 – STEMI involving left circumflex artery
- I21.3 – STEMI, unspecified
- I21.4 – NSTEMI
In most cases, if you report CPT 92941, the main diagnosis should come from I21.
Codes that may support the case, but should not stand alone
Some codes add useful detail about the patient’s condition, but they do not support CPT 92941 on their own. They can help complete the picture, though they should not replace an acute MI diagnosis code.
Examples include:
- I24.9 – acute ischemic heart disease, unspecified
- R07.9 – unspecified chest pain
- I46.9 – cardiac arrest
- I50.9 – heart failure, unspecified
These codes may still matter in the chart. They can show symptoms, severity, or other clinical issues present during the encounter. Even so, none of them by themselves explains why an emergency PCI was performed under CPT 92941.
Note: The key is not just listing heart-related codes. The key is showing that the case involved an acute myocardial infarction. So if CPT 92941 is on the claim, the diagnosis coding should make that fact easy to see. Supporting codes can sit beside it, but they should not take its place.
FAQs
1. Can CPT 92941 be billed with bypass graft PCI codes?
Yes, it can, when the case supports it.
If the interventional cardiologist performs PCI on a coronary artery bypass graft, whether that graft is venous or arterial, the appropriate graft PCI code may be billed along with CPT 92941.
Examples may include:
- 92933 for PCI of a bypass graft
- 92937 for an additional branch of the graft
What matters here is clear documentation. The record should show which vascular segments were native vessels and which were grafted vessels. It should also show that each procedure was medically necessary.
2. Can diagnostic coronary angiography be billed with CPT 92941?
Yes, but not by default.
In many cases, diagnostic coronary angiography is seen as part of the PCI, so it is not automatically paid as a separate service. It may be billed separately only when there is a clear reason it stood apart from the intervention.
That may happen when:
- no prior angiogram is available
- the patient’s clinical status has changed enough to require a new assessment
- the angiographic findings directly shaped the decision to perform the PCI
The key is that the diagnostic coronary angiography must have its own clear purpose. It cannot read like a routine step folded into the PCI.
3. Is manual thrombectomy separately billable?
Usually, no.
When manual aspiration thrombectomy is performed during a PCI billed under CPT 92941, it is considered part of that service. Because of that, it is not billed separately.
The exception is mechanical aspiration thrombectomy. When a mechanical device is used and the documentation supports it, that service may be billed separately under CPT 92973.
This distinction matters more than it may seem at first. Manual aspiration and mechanical thrombectomy are not the same thing, and billing them as if they were can create denials or missed payment.
4. Can PCI in another vessel be billed separately?
Yes, but the coding rules changed in 2026.
CPT 92941 is used for PCI of the culprit vessel during an acute myocardial infarction. If the interventional cardiologist also treats other coronary arteries in the same session, that work may still be reported. The difference is that it now has to be reported with the appropriate primary PCI code, not with the old add-on codes.
That change matters because several add-on codes were deleted for 2026. Those deleted codes include:
- 92921
- 92925
- 92929
So if another vessel is treated, the coding has to follow the current CPT structure rather than the older add-on approach.
5. Does CPT 92941 include moderate sedation?
No, it does not.
When the physician provides moderate sedation during the emergent PCI, that work may be billed separately.
The usual codes are:
- 99152 for the first 15 minutes of intraservice moderate sedation
- 99153 for each additional 15 minutes
The record should show how long the sedation lasted, which medications were given, and what monitoring was performed during that time.