CPT 92937 is a medical billing code. It describes a procedure that restores blood flow in or through a coronary artery bypass graft placed during earlier CABG surgery.
In CABG surgery, a surgeon uses a blood vessel to bypass a blocked artery. However, that graft can narrow or become blocked over time. When this happens, a provider may need to open it to improve blood flow.
This procedure may involve treating the graft itself or passing through it to treat a native coronary artery. It may include stent placement, atherectomy, balloon angioplasty, and embolic protection devices. All of these services are included in CPT 92937.
How Medicare and Insurance Value CPT 92937
CPT 92937 is a complex procedure. Because of that, it takes a high level of skill, careful work, and significant time to perform.
RVU Components (CY 2025–2026)
The Medicare Physician Fee Schedule (MPFS) and industry guides list these work RVUs for CPT 92937:
- CY 2025: 10.95 work RVUs
- CY 2026: 11.30 work RVUs
Overall, this reflects a slight increase in the work RVU for 2026.
Total RVUs for CPT 92937
The total RVUs for CPT 92937 are listed as follows:
- CY 2025: 17.20 total RVUs
- CY 2026: Total RVUs are expected to stay close to the same level, but they will be based on the updated work RVU.
Practice Expense and Malpractice RVUs
For CPT 92937, CMS does not assign separate Practice Expense (PE) and Malpractice (MP) RVU values in the usual way. Instead, the total RVU already includes physician work, along with indirect PE and MP costs.
How RVUs Affect Reimbursement?
RVUs help determine how much Medicare pays for a service. In simple terms, each part reflects a different cost:
- Work RVU covers the physician’s time, skill, effort, and intensity.
- Practice Expense RVU reflects costs such as staff, equipment, and supplies.
- Malpractice RVU reflects professional liability risk.
Next, Medicare adds these values together to get the total RVU. Then CMS multiplies that total by the yearly conversion factor, which is the dollar amount used to calculate payment. As a result, the final number helps determine the physician’s reimbursement.
CPT 92937 RVU Breakdown
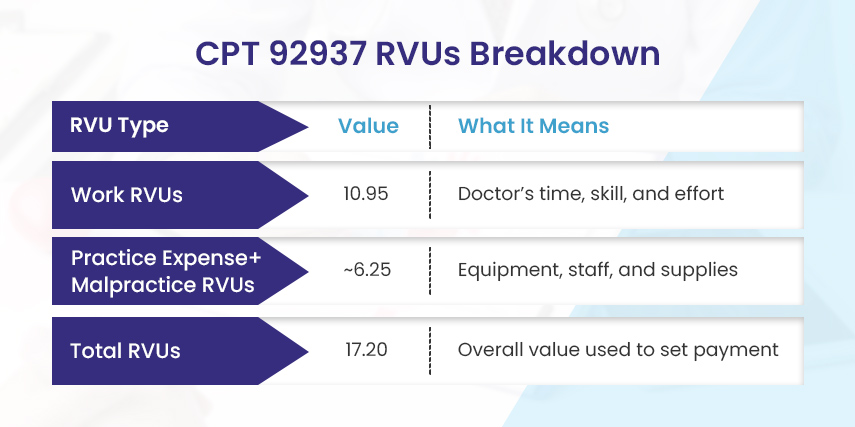
| RVU Type | Value | What It Means |
| Work RVUs | 10.95 | Doctor’s time, skill, and effort |
| Practice Expense+Malpractice RVUs | ~6.25 | Equipment, staff, and supplies |
| Total RVUs | 17.20 | Overall value used to set payment |
What Does Each Insurance Company Pay for CPT 92937?
Insurance companies do not all pay the same amount for CPT 92937. Even though this code has an RVU and a set value, each insurer works out its own payment rate with each doctor and hospital. Because of this, payment can vary by insurer. It can also vary by location.
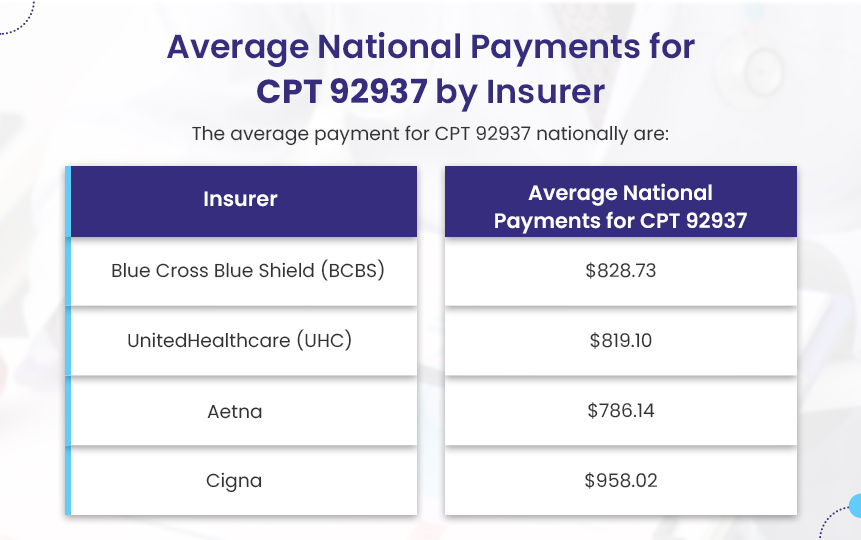
Here are the average national payments for CPT 92937:
- Blue Cross Blue Shield (BCBS): $828.73
- UnitedHealthcare (UHC): $819.10
- Aetna: $786.14
- Cigna: $958.02
However, these are only average amounts. The final payment can still change based on several factors.
For example, the state where you live can affect payment. Also, the place where the procedure is done can change the amount paid. A hospital may receive one rate, while an outpatient center may receive another. This happens because many insurance plans use different payment rates for different types of facilities.
In addition, the provider’s contract with the insurance company plays a major role, especially when working with a cardiology billing company. That contract helps decide how much of the billed amount the insurer will pay for CPT 92937.
CPT Code 92937 Modifiers
CPT modifiers add extra details to a CPT code. They do not change the procedure itself. However, they do tell the insurance company more about the care provided and the situation in which the service took place.
Below are common modifiers used with CPT code 92937.
Modifier 59
Use modifier 59 when the cardiologist treats a bypass graft and a native coronary artery during the same session. Without this modifier, the insurer may view the two codes as the same procedure. As a result, the claim could be denied or reduced.
Modifier 59 tells the insurer that the codes represent two separate procedures on two different vessels. For example, a provider may treat a blocked bypass graft to the right coronary artery (RCA) and also perform balloon angioplasty on a blockage in the native left anterior descending (LAD) artery. In that case, the cardiology surgeon may bill 92937 for the bypass graft and 92920 for the native LAD, with modifier 59 added to one of the codes.
Modifier 76
Use modifier 76 when the same physician repeats the same procedure during the same session. For instance, a cardiologist may treat a bypass graft and then need to return later in the same cath lab session to perform more intervention.
Modifier 77
Use modifier 77 when a different physician repeats the same procedure during the same session. In other words, one physician starts the procedure, and another physician completes or repeats it.
X-Modifiers (XE, XS, XP, XU)
The X-modifiers are more specific versions of modifier 59. Many insurers prefer them because they explain the relationship between the two codes more clearly.
- XE means the services happened during separate encounters, or at different times.
- XS means the services involved separate structures, such as different vessels.
- XP means the services were performed by separate practitioners.
- XU means the service was unusual and did not overlap with the main procedure.
For example, if the provider treats a bypass graft in the morning and then treats a native coronary artery later that day, XE may fit better than modifier 59.
Quick Way to Remember These Modifiers
- 59 or X-modifiers mean: these were separate procedures.
- 76 and 77 mean: the procedure was repeated, either by the same physician or by a different physician.
Add-On Codes Associated With CPT 92937
When a physician treats a blocked bypass graft, CPT 92937 covers the main procedure. However, the physician may also perform extra work during the same session. In those cases, add-on codes help show the full scope of the service.
Add-on codes are extra codes that a provider uses with 92937. They show work that the primary code does not fully describe.
Here are some common add-on codes linked to bypass graft procedures.
92978 and 92979 – Intravascular Ultrasound (IVUS)
These codes describe intravascular ultrasound, or IVUS. With IVUS, the physician uses ultrasound inside the blood vessel to get a clearer view of the blockage. Because these are add-on codes, the provider cannot bill them alone. The provider must bill them with a main intervention code, such as 92937.
92973 – Thrombectomy
Code 92973 describes thrombectomy, which means the physician removes a blood clot during the procedure. A physician may report this code with 92937 or with other coronary intervention codes, such as 92920 through 92928. Again, the cardiology surgeon cannot bill this code by itself.
92974 – Coronary Flow Reserve Measurement
Code 92974 describes coronary flow reserve measurement. This test checks how much blood flows through the coronary arteries after treatment. Like IVUS, the provider cannot bill this code alone. The provider must report it with a main intervention code, such as 92937.
Documentation for CPT 92937
Clear documentation helps support CPT 92937. They show why the patient needed the procedure. They also show what the physician did and how the patient responded. As a result, clear notes can help support medical necessity and payment.
1. Why the Patient Needed the Procedure
The chart should explain why the patient needed treatment. For example, it should list the patient’s symptoms, test results, and level of blockage.
Write down symptoms such as shortness of breath, chest pain, or angina. Also, include the results of the stress test, EKG, and angiogram. Then, record how severe the blockage was.
Example: “Patient presented with unstable angina. Angiography showed an 85% stenosis in a saphenous vein graft to the right coronary artery.”
2. Which Graft the Physician Treated
The chart should also name the graft the physician treated. Some patients have more than one graft. Because of that, the record should be clear.
State the type of graft. It may be a saphenous vein graft, internal mammary artery graft, or radial artery graft. Then, name the target vessel.
Example: “The physician treated the saphenous vein graft to the left anterior descending artery.”
3. What the Physician Used During the Procedure
The record should show what the physician used during the procedure. This helps explain the work and skill involved.
State the type of stent used. Also, note if the physician used balloon angioplasty. In addition, record any atherectomy device used to remove plaque. If needed, include any distal protection device used during the case.
Example: “The physician placed a drug-eluting stent after balloon angioplasty. A distal protection device was also used during treatment.”
4. What the Results Were Before and After the Procedure
The chart should show what changed after treatment. So, record the blockage before and after the procedure.
Write down the percent of stenosis before treatment and after treatment. Next, record the TIMI flow grade. Also, include the images and the written procedure report.
Example: “The pre-procedure stenosis was 80%. After treatment, the residual stenosis was less than 10%, with TIMI 3 flow.”
5. Whether There Were Complications or Extra Devices
The chart should also list any problems or extra devices used. This can support extra coding and show medical need.
Note if the physician performed a thrombectomy to remove a clot. Also, note if the physician used IVUS. If complications occurred, list them clearly, such as perforation, dissection, or arrhythmia.
Example: “Because of a large clot burden, the physician performed mechanical thrombectomy. The physician also used IVUS to check stent expansion.”
Note: The chart should tell the full story of the patient’s condition, the treatment, and the result. In this way, the insurance company can better see the medical necessity of the procedure, understand the work involved, and process payment correctly.
How to Make Sure CPT 92937 Claims Get Paid
You can ensure your claims for CPT 92937 are paid by:
- Using the correct code for bypass grafts, 92937, and for the native coronary arteries, 92920-92928.
- Adding the proper modifiers, such as 59 or an X-modifier, for each of the additional procedures that were performed during the same session.
- Including detailed documentation about the patient’s symptoms, test results, the specific graft(s) that were treated, and pre- and post-treatment results.
- Only submitting add-on codes, such as IVUS (92978/92979), thrombectomy (92973), or coronary flow reserve (92974) when they were actually performed in conjunction with 92937.
- Know what is included in CPT 92937 and do not submit claims for things that are already part of this code.
Easy Checklist Before You Submit a Claim
Before you submit the claim, ask these five questions:
- Did you choose the correct code for the vessel treated?
- Did you add the needed modifiers if the physician treated more than one vessel?
- Does the documentation clearly show medical necessity?
- Are you billing add-on codes only when the physician actually performed them?
- Are you avoiding charges for services already bundled into CPT 92937?
Frequently Asked Questions About CPT 92937
Can I bill 92937 with native artery codes?
Yes, you can bill 92937 with a native artery code when the physician treats both a bypass graft and a native coronary artery in the same session. In that case, report 92937 for the bypass graft and the proper native artery code for the native vessel.
You should also add modifier 59 or the right X-modifier to show that the physician performed two separate procedures.
Does CPT 92937 include distal protection?
Yes, it does. Distal protection devices are included in CPT 92937. So, do not bill for them separately.
How often can I bill 92937 in the same session?
You can bill 92937 for each bypass graft the physician treats in the same session. However, if the physician treats more than one graft, you will need a modifier, such as 59 or XS, to show that each graft was a separate procedure.
What if the physician uses both a stent and an atherectomy?
You still bill 92937 only once for that graft. This is because CPT 92937 already includes the treatment method used during the bypass graft intervention. That includes a stent, balloon, or atherectomy device. In other words, you do not bill extra codes just because the physician used more than one technique.



