Do you have trouble with cardiology billing because you feel like coding systems and payers are creating an endless web of confusion?
If so, you have found the right resource!
CPT 92924 is likely one of the most difficult and most important codes when performing Interventional Cardiology billing. This code defines coronary atherectomy (CA) which is performed at the same time as an angioplasty. The importance of this code lies in its ability to be used as the code for all complicated cases that require placement of anything other than a standard stent.
In addition, CPT 92924 provides both a higher level of reimbursement and stricter compliance than any other stent-related code. Therefore, if you fail to accurately document and submit the 92924 code, you may lose valuable reimbursement dollars by way of denied claims or even potential audits.
Here’s an easy-to-use guide to assist you in learning more about CPT 92924:
Description of CPT Code 92924
CPT Code 92924 refers to an atherectomy, a procedure to either remove or modify blockages within coronary arteries. The process involves the use of a catheter to remove (or modify) plaque from the artery walls to improve blood flow through the artery. By 2026, CPT Code 92924 will provide documentation for reporting an atherectomy performed on one major coronary artery segment including its associated side branches (i.e., the right coronary artery, the left anterior descending artery, and the circumflex artery).
In some cases, the physician may perform an angioplasty by means of balloon to further open the narrowed coronary artery and enhance the atherectomy results, but since balloon angioplasty is a component of the atherectomy, the balloon angioplasty does not need to be separately documented. Therefore, CPT Code 92924 documents a coronary artery procedure that is focused upon one arterial location and was primarily accomplished by the method of atherectomy. Balloon dilatation was used as necessary to achieve optimal results.
Type: Interventional Cardiology (PCI Code Group)
CPT Code 92924 is a member of Interventional Cardiology and therefore is designated as a PCI code group. PCI Codes represent a grouping of small interventional cardiac procedures intended to restore adequate blood flow through the coronary arteries. PCI codes are typically performed in a special laboratory environment equipped with various types of catheters to facilitate the opening of obstructed or stenosed coronary arteries. Consider PCI as a “tool box” for opening coronary arteries and CPT Code 92924 as just one tool found within this “box”.
Here are some other common PCI codes you might see with 92924:
- 92928 means putting a stent in the coronary artery, and it includes angioplasty if it is done.
- 92933 means doing an atherectomy with putting in a stent, and it also includes angioplasty if it is done.
- 92920 means balloon angioplasty by itself when there is no atherectomy or stent used.
These codes help the medical coder know what specific procedure(s) were done during the intervention, whether the doctor used a balloon, a stent, an atherectomy device, or a mix of these devices.
One important update for 2026 about PCI services is how PCI services are set up for reporting. PCI codes are now shown as base codes, which stand for main coronary artery areas; the old way of reporting branch add-on work separately is not used anymore. The base codes have been changed to show the work done in the branches of the treated major coronary artery.
For example, if the doctor does atherectomy and balloon angioplasty in the left anterior descending artery area, but also treats a diagonal branch that comes from the left anterior descending artery. If you use the same kind of PCI work, you would report the basic PCI code under the 2026 reporting structure. For the left anterior descending area, you would not add a different branch code, even if the diagonal branch was treated. This work in the branch is considered part of the area-based base code.
When to report CPT 92924 in clinical use
CPT 92924 is reported when a cardiologist does an atherectomy on a heavily calcified or complicated blockage in a coronary artery. Sometimes, balloon angioplasty by itself will not fully open the vessel. The calcified plaque might be too strong to let a stent go in, or it could get big enough for the stent to fit right. Atherectomy is a way to prepare the artery by modifying the plaque. This helps to make the vessel wider and allows for stent placement if needed.
Documentation note: Atherectomy is a more intense PCI service compared to regular balloon angioplasty with possible stenting. The chart should clearly show the additional reason(s) for the extra work done for the patient.
Write down how much calcification is in the lesion and also note how complex the blockage is. Remember that balloon angioplasty by itself is not enough because it can’t fully open the vessel.
Also, explain why doctors choose atherectomy instead of just balloon angioplasty. These reasons show why this extra service is needed.
Coding Guidelines for 92924 CPT Code in 2026
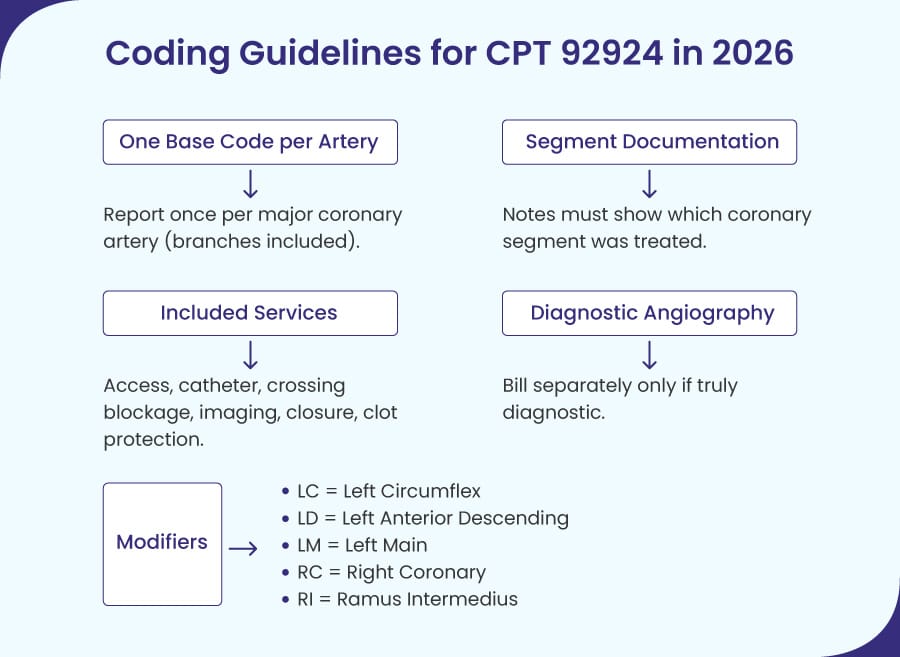
1). Limit Reporting to One Base Code Per Territory
Starting in 2026, CPT 92924 will be the main code for coronary atherectomy and can be billed only one time for each major coronary artery area. Any branches handled in this area can also be part of the report for this base code. If more than one PCI procedure happens in the same area, you only report one base code (the most intensive PCI procedure), no matter how many services were given. If coronary atherectomy is done in that area, 92924 will cover all PCI work for that area instead of just the simpler option of angioplasty alone.
2). Document Coronary Segments Using Standard Models
When reporting 92924, the provider’s notes should say which coronary parts were treated and should follow a known segment model to show which main area was treated. This is needed to explain any extra work done by the doctor in the branch areas of the main territory since the 2026 removal of Branch Add-on codes.
3). Bundle Routine Services into the Primary Procedure
In billing for 92924, the doctor usually includes the main parts of the PCI procedure. This covers: getting access to the blood vessel, using a catheter, crossing the blockage, overseeing and interpreting images, closing the access point, using protection against clots if needed, and imaging to show the PCI procedure is done. These parts are usually not reported separately just because they happen with the atherectomy procedure.
4). Restrict Separate Billing for Diagnostic Angiography
Diagnostic coronary angiography done in the same session as 92924 cannot be billed separately by default. It is usually reportable only when it fits the definition of diagnostic. This happens when there isn’t a good angiograph available beforehand, and the test done that day makes the doctor decide to treat, or when the patient’s condition requires a new test.
5). Append Anatomical Modifiers to Identify Territories
When reporting 92924, choose the coronary artery modifier that fits the major coronary area treated:
- LC means Left Circumflex
- LD means Left Anterior Descending.
- LM means Left Main
- RC means Right Coronary
- RI means Ramus Intermedius
Medicare 2026 Fee Schedules for CPT 92924 (National Averages)
The amounts shown below are the national averages for Medicare costs allowed for CPT 92924 in a facility, according to the Physician Fee Schedule for 2026. The real allowed cost might be different from the national average because of local area changes. Also, there might be other claims-related things or paperwork problems that can impact payment.
Payment for facilities under Medicare PFS
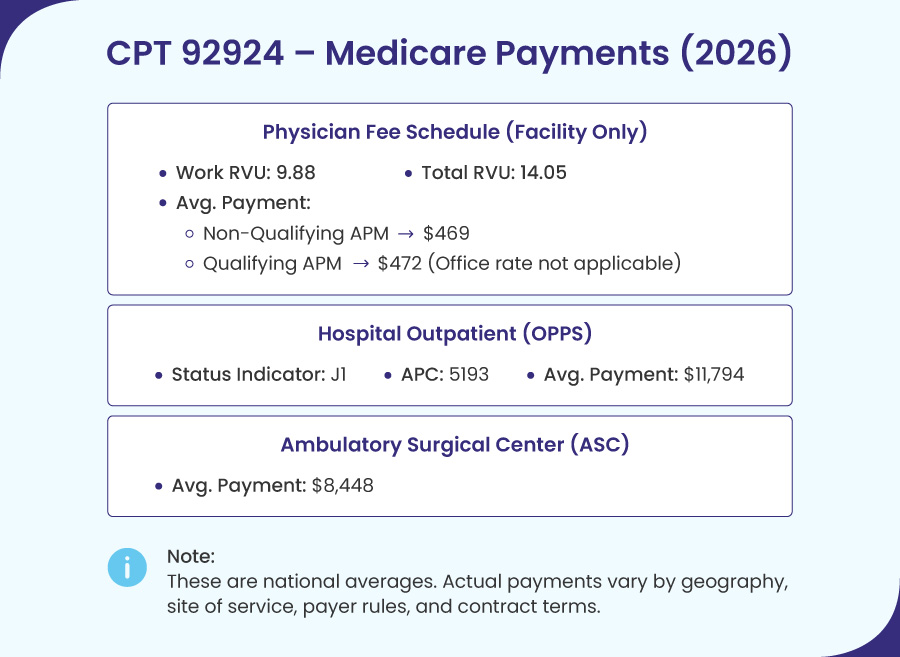
In 2026, the values for CPT 92924 show:
- Work RVU: 9.88
- Total facility RVU is 14.05.
- About the national average payment for Medicare doctors (in a facility): $469
- This service is not done in an office, so the office rate does not apply.
Conversion Factors for 2026
- Conversion Factor for Qualifying APM is 33.5675
- Conversion Factor for Non-Qualifying APM: 33.4009
Medicare calculates doctor payments by multiplying the service’s Total RVUs with the Conversion Factor. Geographic adjustments are then applied to the result.
- CF Non-qualifying APM: 14.05 x 33.4009 ≈ $469.28, or about $469
- CF Qualifying APM: 14.05 x 33.5675 ≈ $471.62, or about $472
Note: These are “National Averages”; local changes and/or payer rules can raise or lower the actual amount paid to the provider. The numbers above show what doctors get paid under the PFS in a facility, but they do not show the total hospital payment for the procedure.
Payments for CPT 92924 at Hospital Outpatient and Ambulatory Surgical Center (ASC) in 2026
CPT 92924 will be seen as a complete service when billed through a hospital outpatient department using OPPS under Medicare in 2026. CPT 92924 has a status indicator of “J1”. The J1 status indicator is used by Medicare to show what the payment is for the visit and all the related services on that day. Most services for CPT 92924 will be included in the single payment for the CPT 92924 procedure. APC 5193 is assigned to CPT 92924 for OPPS payments. The national average OPPS payment for this APC in 2026 is $11,794.
In an ambulatory surgical center (ASC), Medicare will pay for CPT 92924 in a different way under its ASC payment rules. In 2026, the average ASC payment for CPT 92924 is $8,448.
There are national averages for paying for procedures like CPT 92924. However, like other medical care, many factors can change for each patient treated at an ASC or hospital outpatient facility. Examples are site of service rules, local and contract issues, and possible payer edits.
Also, commercial payers can have different rules about paying for CPT 92924 at an ASC. So, it is a good idea to check the exact policy of the commercial payer before using the Medicare payment amount for CPT 92924 as a guide for your patient’s treatment.
Modifiers and Add-On Codes for CPT 92924
The usual questions from payers about CPT 92924 on a claim are: “which major coronary artery territory was treated?” Starting in 2026, the territory-based method will be part of the PCI code system. So, modifiers will hold a lot of the information needed to explain where the procedure happened to help it go through the payer’s systems easily. The PCI base codes were updated to cover work in branches of the main artery. Because of this, older branch add-ons found online might confuse coders when coding for 2026.

1). The coronary artery territory modifier is the primary modifier for CPT 92924.
The claim line usually has the coronary artery modifier linked to the treated major area, like this:
- LD means left anterior descending.
- LC means left circumflex.
- LM means left main.
- RC means right coronary
- RI means ramus intermedius
So, practically speaking, the territory modifier (LD) will be 92924 when the atherectomy is performed in the LAD area, or 92924 with (RC) when it is done in the RCA area. That’s important to know, since this territory modifier provides the site context that many payers require for PCI claims and reduces the amount of “missing site” edit delays.
Another 2026 recommendation that works well with 92924 is that while the documentation can mention the territory name; the documentation needs to describe where the segment or lesion is in relation to the territory using the standard coronary segment model used to report PCI.
2). Distinct modifiers appear with CPT 92924 only when something is really separate.
Distinct modifiers for CPT 92924 are reported only when another service is reported on the same date and an edit needs proof that two services were given.
Usually, most 92924 claims need just the coronary artery modifier. But, when another service is reported on the same date, and a bundling edit needs proof that the two services did not overlap, using different modifiers is important.
CMS suggests using the X modifiers when you can:
- XS = separate structure
- XE = separate
- XP = separate
- XU = unusual non-overlapping service
Modifier 59 is still there, but CMS says to use it only when none of the X modifiers clearly explain the service being reported as separate.
3). The 2026 change that impacts CPT 92924 is the removal of branch add-on PCI codes.
Branch add-on PCI codes have been in PCI guidelines for many years. In 2026, the branch add-on PCI codes were removed, and the main PCI codes were updated to cover work in branches of the main coronary artery that was treated.
This means that in a 92924 situation, if atherectomy is done in a main coronary area and more PCI work is done in a part of that area at the same time, you usually use one base code for that area. The paperwork shows all the work done instead of needing a separate branch add-on PCI code.
4). Codes that might show up on the same date as CPT 92924 are not branch add-ons, but they still need to be valid on their own.
Even though branch add‑on PCI codes are no longer used, CPT 92924 may still be reported when other services are performed and documented as separate. One common example is coronary physiology assessment, with codes 93571 and 93572, which remain subject to payer rules and bundling guidelines.
A helpful reminder to think about is that “performed in the room” is not the same as “can be billed separately.” The paperwork must clearly show that the companion service meets the rules for separate billing according to the payer’s guidelines.
Quick Takeaway
For CPT 92924 in 2026, focus on the coronary area first:
- Choose the right PCI base code for the treated major coronary artery area.
- Attach the right coronary artery modifier (LD/LC/LM/RC/RI).
- Only use 59 or X{EPSU} when you have proof of a service that is really different and a payer edit needs it.
Tips for Documentation and Compliance

Understand the documentation and compliance for 92924 CPT Code can make medical billing easier for this procedure if your documentation clearly explains the patient’s case. Your documentation should read like a clear story that answers the following questions easily for reviewers, so they don’t have to search for them.
- Why did the doctor have to do an atherectomy?
- Where was the atherectomy treatment performed?
- What was done during the treatment?
The clearer your documentation is about the questions above, the quicker the denial or audit process usually goes. Clear documentation on the above questions makes the denial or audit process go more smoothly.
Establish Medical Necessity for Atherectomy
The payer needs to see proof that the doctor picked the atherectomy procedure for a specific reason related to the lesion, not just because of personal choice, since CPT 92924 is for an atherectomy procedure. Your documentation will work best when it clearly shows what made the lesion difficult to treat and why atherectomy was the right choice over other options.
Some common documents that might give more details to back up the medical necessity for CPT 92924 include:
- Calcified lesion
- Tight or resistant lesion
- Lesion had complex anatomy
- Doctors thought that the balloon angioplasty would not open the blockage enough.
- The main goal of the atherectomy procedure is to get the lesion ready for a safer or better result with the next percutaneous coronary intervention (PCI).
Define Treated Territories and Anatomical Modifiers
In 2026, CPT 92924 is coded by the main coronary artery area. Work done in branch vessels is usually part of the service for that main coronary artery area. So, noting where the service took place (coronary artery area) and using the coronary artery modifier is very important for the documentation needed for CPT 92924.
The documents need to show the following clearly:
- The main coronary artery area is being treated with the modifier linked to that area.
- Location of the segment or lesion in the area being treated is described clearly and consistently.
Recognize Components Bundled into CPT 92924
Your documentation must explain the procedures done, but it should not suggest separate services from other procedures included in CPT 92924.
Here are two reminders to help you avoid common mistakes in this area:
- If CPT 92924 is done, any balloon angioplasty in the same area should be counted as part of the service.
- Many usual steps in a percutaneous coronary intervention (PCI) are automatically added. These typically cover vascular access, crossing the lesion, imaging to confirm completion, and closure using the access sheath.
Document by Territory Rather than Lesion Count
A common mistake in documentation happens when doctors focus on how many lesions they treat instead of how to report percutaneous coronary interventions in 2026.
Key Points To Consider For CPT 92924
For procedures with one major coronary artery area, the paperwork should show one main code that reflects the most intense service given in that area, which is CPT 92924 if atherectomy is the main service.
If two different major coronary artery areas are treated in the same session, it may be necessary to report them separately. This is only if the documentation shows that two separate areas were treated and the modifiers used with the separate codes accurately represent each area.
Validate the Independence of Diagnostic Angiography
Denials often happen when billing for diagnostic coronary angiography on the same day as CPT 92924, unless the paperwork clearly shows that the diagnostic study was truly diagnostic and not just part of the interventional process.
Examples of documents that would show the diagnostic coronary angiography was really diagnostic include:
- Reasons to do a diagnostic study that day
- Clear test results that led to the choice to go ahead with a procedure
Align Diagnosis Coding with the Clinical Narrative
CPT 92924 usually has a special reason based on clinical signs like calcification or how tough the lesion is. When the paperwork gives more details, diagnosis coding that matches the clinical picture usually relates to how complex the atherectomy is.
When do denials and audits affect CPT 92924?
There are many usual places where denials and audits on CPT 92924 happen. Knowing these possible problem spots when making your documentation can help cut down on extra work.
Here are common mistakes to avoid:
- The coronary artery modifier is either missing or wrong for the area that was treated.
- The documents show that stenting happened in the same area as the CPT 92924 procedure, but CPT 92924 was billed instead of the correct code for stenting.
- The bill for the coronary angiography was sent without a clear reason for doing the test.
- Regular use of distinct modifiers without enough proof/documentation to show a different service.