As cardiovascular treatments and procedures increase, accurate medical coding is very important to ensure fair reimbursement and stay compliant with payer policies.
Every cardiology billing firm should know that CPT Code 92933 is important for proper documentation and billing for Advanced PCI (Percutaneous Coronary Interventions). This is because this procedure code helps cardiologists get paid fairly for the extra skill, equipment, and time needed for plaque removal (atherectomy) and putting in stents.
92933 CPT Code Billing Guide & Description
CPT code 92933 refers to a procedure called percutaneous transluminal coronary atherectomy with intracoronary stent placement, with coronary angioplasty when performed, in a single major coronary artery or branch.
In simple words, this medical code is applied when doctors remove blockages in a coronary artery using a special tool and place a stent. This may also include widening the artery if needed, and it is done in one major coronary artery or its branch.
- Atherectomy is when plaque is taken out from the walls of arteries.
- Stent placement means putting a support device into the artery to keep it open.
Since 92933 describes a specific heart procedure (atherectomy + stent, with angioplasty if done), it has its own CPT code for clear reporting and billing.
CPT 92933 Fee Schedule (Last checked: February 2026)
Getting paid for CPT 92933 will depend on several factors. These include what the insurance companies have agreed to with the providers, where the procedure was done, how the provider is sending the claim (whether it’s a doctor or a hospital), and the rules for coding and billing that apply.
Note: CPT 92933 is a code for a procedure called PCI (coronary intervention), not for evaluation and management (E/M). It is not chosen based on the level of medical decision making, like moderate MDM.
Key points to remember (for getting reimbursed):
- Claims and “site of service” matter. Physician claims are billed in a different way than hospital claims. Claims from physicians are paid under the Physician Fee Schedule (PFS) if the patient is either staying in the hospital or visiting as an out-patient (Patient’s Place of Service = POS 21/19/22).
- Payments for hospital inpatient care do not come from the CPT-based Physician Fee Schedule.
- Medicare uses the IPPS/MS-DRG method to decide how much to pay for hospital stays.
- Payments for Hospital Outpatient Facilities are done using the OPPS/APC method. The use of PCI codes can vary based on how you coded it, like whether it’s for a non-drug eluting or drug eluting stent.
- The amount of reimbursement a provider gets for a service can be affected by several things. These include the agreements between the payer and the provider, whether the service was done in a hospital, how the service was sent to the payer (by a doctor or a facility), and where the provider and the payer are located.
- Medicare PFS Tools are made for Medicare and change depending on the local area.
- Use the right modifiers and documentation when needed (For example: Coronary Artery Modifiers – LC, LD, LM, RC, RI)
Average Reimbursement Rates for CPT 92933 from Major Insurance Payers
Each payer’s agreement and policy determine the amount each payer pays for CPT 92933 to the cardiologist.
| Payer | Average Reimbursement |
| Blue Cross Blue (BCBS) | $935.90 |
| United Health Care (UHC) | $918.50 |
| Aetna | $882.87 |
| Cigna | $1,073.11 |
Cigna pays approximately $1073.11 for CPT 92933. Compared to other payers, Cigna pays better for more complicated PCI cases. This is because Cigna covers so many patients, and therefore, provides a way for providers to earn more money.
Aetna has the lowest average payment for CPT 92933, which is $882.87. Depending upon the number of Aetna patients a hospital has, it may experience less reimbursements due to the lower payment for CPT 92933.
UnitedHealthcare and Blue Cross Blue Shield pay roughly the same as each other, which is $920 to $935 for CPT 92933. Because UnitedHealthcare and Blue Cross Blue Shield offer moderately high payment levels, and relatively consistent payment levels, the two payers can be considered mid-range.
Why There Are Differences in Payment Levels for CPT 92933?
Each payer determines the amount it will pay for a particular service, including CPT 92933, through a process that includes negotiations, contract development, cost determination of performing PCI services in various regions, and establishing guidelines for the performance of complex PCI services.
Because atherectomy and stent placement are included in the CPT 92933 code, payers typically place a greater premium on the increased complexity associated with the completion of both procedures. As such, hospitals and providers frequently experience wide variations in their revenue generation as a result of the types of patients they treat and the agreements they enter into with payers.
Therefore, a cardiology practice that serves primarily Cigna patients can anticipate receiving $1073.11 per case, while a cardiology practice that serves primarily Aetna patients should anticipate receiving significantly less, approximately $882.87 per case.
Correct coding and proper documentation enables providers to take advantage of the full payment for each procedure when using CPT 92933. Providers run the risk of being reimbursed improperly if they incorrectly document or report the procedure (i.e., incorrectly documenting as CPT 92928, “Stent Only”, rather than properly documenting as CPT 92933).
As such, cardiology billing firms that are knowledgeable regarding current payment trends and schedules from multiple payers are well-equipped to manage the cash flow for cardiology practices, and create better contracts that adhere to all applicable laws and regulations.
2026 PCI Coding Update Note: In 2026, changes to the CPT PCI codes took place. Work completed within one main coronary artery or its branches is now documented using one code. Certain PCI branch add-on codes (such as CPT 92934), were deleted in this change.
Importance Of Effectively Using 92933 CPT Code for Cardiology Reimbursements
Utilizing CPT 92933 effectively will have a substantial effect on the monies, rules, and preparedness of healthcare providers for audit, and therefore will be an important code in heart-related billing:
- Properly using 92933 CPT code to document the complex procedure of atherectomy and intracoronary stenting will assist in preventing under-coding, payment denial, and low reimbursement for the healthcare provider.
- Incorrect billing methods (i.e., using the incorrect code – for example using CPT 92928, for stenting, rather than using CPT 92933 for both atherectomy and stenting), may decrease the amount of money received by the healthcare provider.
- Incorrect billing methods (i.e., over-coding – for example using CPT 92933 for only atherectomy) may increase the likelihood of claims being denied and audited. In such instances, the coder should utilize either the atherectomy-only PCI code (i.e., 92924, if applicable), or another PCI code (other than 92934), which accurately reflects the procedures performed. The PCI add-on codes were eliminated in the 2026 PCI coding update.
- The paper work must be complete, and the operative note must clearly outline which coronary artery was treated, and the operative note must detail that atherectomy with intracoronary stent placement (and angioplasty, if performed), was completed, along with a description of the necessity for the procedure. This will enable the payers to review the documentation related to authorization.
Modifiers Applicable to 92933
The CPT Code 92933 does not represent all coronary interventions; it is a PCI Code that represents coronary atherectomy with intracoronary stent placement (with coronary angioplasty when performed) in one major coronary artery and/or branches (PCI Coding Convention 2026). PCI situations other than described above would use other CPT/HCPCS codes (for example, only angioplasty or stent only intervention).
Modifier Codes for Coronary Arteries help to describe the coronary artery being treated. Most commercial payers and government agencies (like Medicare) require accurate coronary artery modifiers on all PCI claims and failure to enter an appropriate coronary artery modifier can lead to claim edits/denials based upon the payer’s rules.
Some examples of coronary artery modifier codes (used in conjunction with PCI codes – and specifically 92933, when possible) include:
LD – Left Anterior Descending (LAD) coronary artery
Most commonly treated and provides oxygenated blood to the majority of the Heart Muscle. The “LD” modifier should be used when the treated vessel is the Left Anterior Descending coronary artery.
Example: An atherectomy with intracoronary stent placement is performed in the LAD, report 92933-LD (payer formats will vary).
RC – Right Coronary Artery (RCA)
The right Coronary Artery (RC) supplies oxygenated blood to the right side of the body that makes up the heart. The “RC” modifier should be used by the physician when the treated vessel is the Right Coronary Artery.
Example: An atherectomy with intracoronary stent placement is performed in the RCA, report 92933-RC.
LC – Left Circumflex (LCX) coronary artery
Left Circumflex supplies oxygenated blood to the lateral and posterior walls of the body that make up the heart. The “LC” Modifier should be used by physicians when the treated vessel is the Left Circumflex coronary artery.
Example: An atherectomy with intracoronary stent placement is performed in the LCX, report 92933-LC.
LM – Left Main coronary artery
When reporting the “Left Main” modifier, the physician has performed either atherectomy or placed stents in the area of the coronary arteries where the Left Anterior Descending (LAD), and the Left Circumflex (LCX) branches originate – this is the origin of the Left Main Coronary Artery.
Example: An atherectomy with intracoronary stent placement is performed in the left main coronary artery → report 92933-LM.
RI – Ramus Intermedius coronary artery
Physicians add the “RI” modifier when the treated vessel is the Ramus Intermedius.
Example: An atherectomy with intracoronary stent placement is performed in the Ramus Intermedius → report 92933-RI.
Common CPT 92933 Coding Issues and Solutions
When reporting CPT 92933, use it only when coronary atherectomy with intracoronary stent placement (with coronary angioplasty when performed) is documented. Under 2026 PCI coding conventions, work performed in a single major coronary artery and/or its branches is reported with a single code, so documentation and artery modifier reporting (when required by payer policy) must accurately support the service reported.
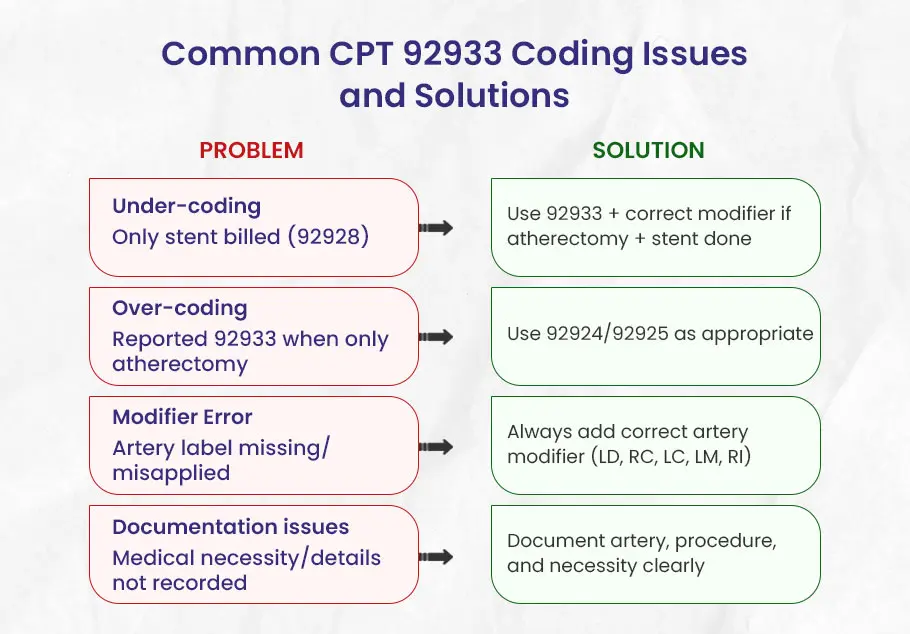
There are several common issues that may arise regarding CPT 92933. Some of them are listed below:
1). “Only Reporting the Stent” (Under-coding)
Claims have been submitted using 92928 (only stent) when the physician performed both an atherectomy and stent placement. This under-reports the total scope of the procedure and results in reduced reimbursement for the physician’s services as well as de-values the service rendered by the physician.
How to Fix the Problem:
Carefully review the operative note to confirm that both atherectomy and intracoronary stent placement were performed and documented in the same major coronary artery and/or its branches (per 2026 PCI coding conventions).
When required by payer policy, report the appropriate coronary artery modifier (for example, 92933-RC for the right coronary artery) to support correct claim adjudication; modifier use helps reduce edits/denials but does not guarantee payment.
2). “Coding More Than Was Done” (Over-coding)
CPT 92933 describes coronary atherectomy with intracoronary stent placement (with angioplasty when performed) in a single major coronary artery and/or its branches.
If the physician performed only an Atherectomy and did not place a stent then reporting 92933 would be incorrect because it describes a more complex service than was performed.
This type of error is considered Over-Coding because the reported code contains a procedural element (Stent Placement) that was not performed or documented. These types of errors can cause claim denial, audits and compliance risk.
How to Fix the Problem:
Report the code that accurately describes the procedure documented on the operative report. If only an atherectomy was performed in the left anterior descending (lad) and no stent was placed the appropriate code for this procedure is:
92924-LD (percutaneous transluminal coronary atherectomy, with coronary angioplasty when performed; single major coronary artery or branch)
Do not report 92925 for 2026 coding and later, because 92925 was deleted. Under 2026 PCI coding conventions, work in a single major coronary artery and/or its branches is reported with a single base code (for atherectomy-only scenarios, use the appropriate current base code such as 92924, when supported by documentation).
3). “Omitting the Artery Label” (Modifier Error)
The artery-specific modifier (LD, RC, LC, LM, RI) is either omitted or misapplied. Many payer rules (including Medicare contractor PCI billing guidance) require a coronary artery modifier to identify the treated vessel, and omission/misapplication may lead to claim edits, delays, or denials. Reimbursement will be delayed and additional correspondence may be required.
How to Fix the Problem:
Always include the correct modifier based upon the operative note. For example: atherectomy + stent in LCX → 92933 LC.
4). “Missing the Why” (Documentation Issues)
A common documentation issue is failing to clearly record medical necessity and the key procedural details that support the code reported.
The operative note does not document the mdedical necessity of the procedure nor the details of what was done during the procedure.
If the record does not support medical necessity and the performed intervention, payers may deny the claim or request additional documentation. Detailed documentation of the procedure is necessary for payers to understand why a complex procedure such as atherectomy + stent was medically necessary.
How to Fix the Problem:
Document thoroughly:
- Which artery was treated
- An atherectomy and stenting have been performed
- The need for this procedure was medically necessary (e.g. Severe Stenosis requiring Intervention).
For Example: Atherectomy performed on Right Coronary Artery followed by Stenting due to Severe Stenosis → Supports Billing for 92933 RC.
FAQ’s
Is there any documentation that I need to provide for CPT Code 92933?
In order to document CPT code 92933 correctly, you will be required to create detailed operative reports of the atherectomy with stent placement procedure that include:
- The name of the artery being treated.
- That both atherectomy and intracoronary stent placement were performed and documented in the same major coronary artery and/or its branches (per 2026 PCI coding conventions).
- Medical necessity for completing these interventions.
Can CPT 92933 be billed for every artery treated?
It can be reported for each separately treated major coronary artery (when the documented service meets the 92933 descriptor), but not simply for every branch within the same major artery. Under 2026 PCI coding conventions, only one base PCI code is reported for revascularization of a major coronary artery and/or its branches.
Also, use the correct coronary artery modifier when required by payer policy (for example, LD, LC, RC, LM, RI — not “RCA”). Medicare PCI billing guidance states claims for PCI must include the appropriate vessel modifier.
Example: If atherectomy with intracoronary stent placement is performed in the LAD, report 92933-LD (when payer policy requires a coronary artery modifier). If the same type of intervention is performed in the right coronary artery, use the modifier RC (report 92933-RC), not “RCA.”
What will happen if CPT 92933 is miscoded?
Miscoding CPT 92933 can cause many problems such as loss of revenue, claim denial, etc. If you undercode the service (you use 92928 for a stent only when an atherectomy was also performed), you will receive less reimbursement for that service. Overcoding the service (for example, reporting 92933 when only atherectomy without intracoronary stent placement was performed) increases denial and audit risk. In that scenario, the coder should report the atherectomy-only PCI code (such as 92924, when supported by documentation) rather than 92933. Also, 92934 was an additional-branch atherectomy + stent code and was deleted for 2026, so it is not the correct code for “atherectomy only.”
How will CPT 92933 impact Cardiology Billing?
CPT 92933 affects cardiology billing because it supports accurate reporting of a PCI service that includes atherectomy plus intracoronary stent placement (with angioplasty when performed). Accurate coding, modifier use (when required), and documentation can help reduce undercoding/overcoding, denials, and compliance risk, but payment still depends on payer rules and contracts.