Key Takeaways:
Start right: Observation billing starts only with a proper outpatient observation order and a documented time of start.
Bill wisely: Only count active observation hours, not waiting or recovery hours.
Code properly: Use G0378 for hours, G0379 for direct admissions and pair with revenue code 0762.
Know OPPS regulations: Medicare pays separately only if observation lasts 8 or more hours and links to a qualifying visit.
Be compliant: Make sure to use clear wording in your orders, provide the MOON in a timely manner, and apply Condition Code 44 when an inpatient case is changed to outpatient.
You want to code correctly to comply with the CMS mandates and to avoid denials. This guide will show you how to bill outpatient observation services correctly. It covers CMS guidelines for observation billing, observation charge rules, the Medicare observation time frame, and the observation CPT/HCPCS codes.
Step-by-Step Guide to Billing Outpatient Observation Service
Billing for outpatient observation can be tricky, but it comes down to knowing when the clock starts, which hours count, and how Medicare wants them coded. This guide breaks down the CMS rules into clear steps so you can follow along without second guessing.
1). When Does Observation Start
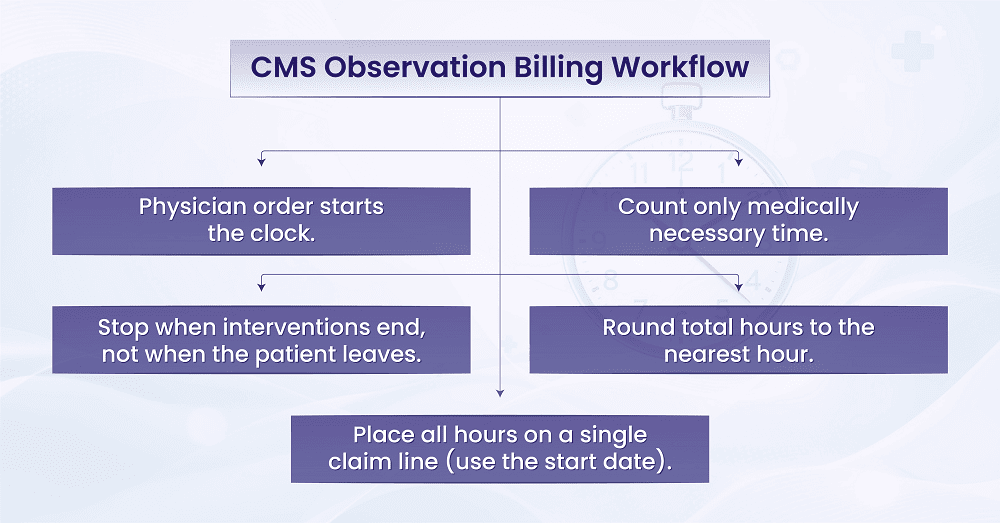
Observation is an outpatient hospital service that starts with the order of a physician (or other qualified provider). The time of the order becomes the start of observation by using the documented time in the medical record. More specifically, the billing clock doesn’t start until, and unless, documentation demonstrates that observation care was initiated.
Example: If a doctor writes an order at 2:15 p.m. and the nurse documents that observation began at that time, then 2:15 p.m. is the official start. Even if the patient was in the ED for several hours before, those earlier hours do not count.
2). Moving From Start Time to What Hours Count
Once you know when to begin, the next step is figuring out which hours are billable. You should bill only for hours when staff are administering observation care or for other medically necessary services. If the team is still providing follow-up treatment even after a discharge order, those hours can also be billed. However, time spent waiting for a ride, waiting for a bed, or engaging in other nonclinical activity cannot be used to generate billable hours.
Example: A patient’s discharge order is written at 9:00 a.m., but the nurse continues to check vitals and provide IV fluids until 10:00 a.m. That extra hour counts. If the patient then waits in the lobby until noon for a family member, those two hours do not count.
3). From Total Hours to the Reportable Units
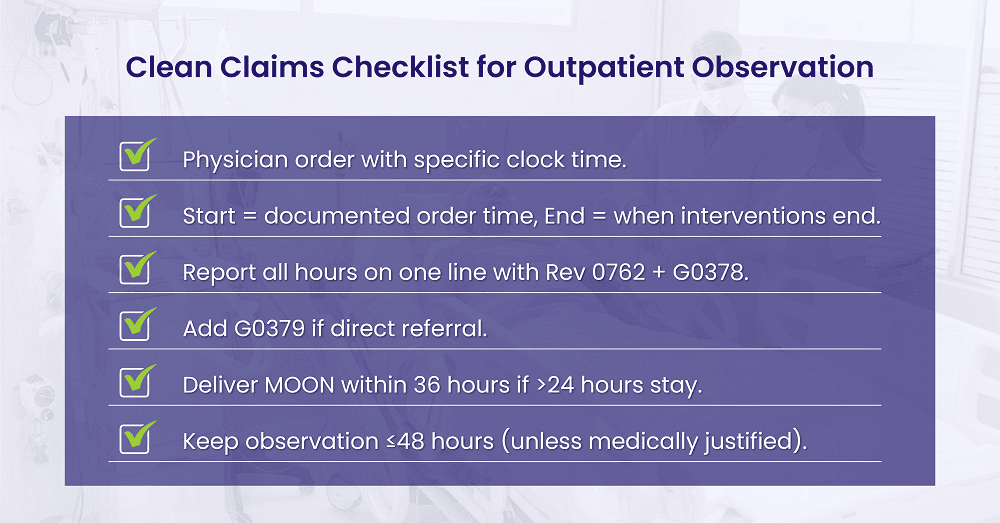
After calculating total hours, CMS asks that you round to the nearest hour. Then, report those rounded hours using G0378 units on the claim. If the stay extends past midnight, all observation hours count on one claim line report, and you use the date observation began as the date of service for that line.
Example: A patient is in observation from 11:10 a.m. until 7:40 p.m. That is 8 hours and 30 minutes, which rounds up to 9 hours. You would report 9 units of G0378. Even if that stay went overnight, you would still place all hours on one line with the start date as the service date.
4). Linking to Situations Where You Should Not Bill
It is just as valuable to understand when observation billing is not applicable. Observation should not be viewed as a holding area for routine post-surgical care. Furthermore, observation cannot be billed at the same time as a procedure or test that includes active monitoring. Thus, if there is a break in the observation stay due to a procedure, you must separate and document the time spent in the procedure before summing the remaining observation hours.
Example: A patient is placed in observation at 3:00 p.m. At 5:00 p.m., the patient goes to radiology for a procedure that takes one hour and includes monitoring by the radiology team. Observation time pauses at 5:00 p.m. and resumes at 6:00 p.m. So, if the patient leaves at 10:00 p.m., you can bill for 6 hours of observation (3:00–5:00 p.m. and 6:00–10:00 p.m.).
5). Transitioning Into Payment Rules
Now that you know what time counts, your next question is how Medicare payment will be provided. Under the outpatient prospective payment system (OPPS), observation will be paid as a separate service, but only if certain conditions are met. In normal cases, this requires a qualifying ED visit, clinic visit, critical care visit, or direct referral to observation services, and at least 8 billed hours of G0378.
6). What Happens If the Rules Are Not Met
If those conditions are not met, observation is packaged into the payment for other outpatient services. For example, if a T-status surgery is performed on the same day, observation will not receive a separate payment. However, you should still bill observation hours, because the OPPS logic determines whether to package or create payment.
Example: If a patient is placed in observation for only 5 hours after an ED visit, Medicare will not pay separately for observation. Instead, the cost of those 5 hours is bundled into the payment for the ED visit.
7). Wrapping Up With the MOON Requirement
Finally, in a case with a Medicare patient kept in observation for greater than 24 hours, hospitals and CAHs must provide the Medicare Outpatient Observation Notice (MOON). This notice must be provided to the patient within 36 hours after initiation of observation, and earlier if the patient is discharged, admitted, or transferred. The signed notice must, at all costs, be kept in the record.
Example: A patient has been in observation since Monday at 2:00 p.m. If the patient is still in observation on Tuesday at 4:00 p.m., the MOON must already have been delivered by that time. If the patient is discharged Tuesday morning at 10:00 a.m., then the MOON must be given before discharge.
Observation CPT and HCPCS Codes and Revenue Code
Start with G0378 when billing for observation time. This code is billed per hour, based on the total rounded hours the patient spends under observation. Always pair it with revenue code 0762 on the UB-04 claim because they belong together.
If the patient comes directly from the community, meaning they were not first seen in the emergency department or clinic, you should also add G0379 on a separate line. This code shows that the patient was a direct admission to observation. Keep in mind that G0379 is a hospital facility code, not a professional service code.
Most hospital outpatient observation claims use Type of Bill 13X. Critical Access Hospitals (CAHs) should use 85X. If your facility type is different, check the payer’s policy to confirm which bill type applies.
The Smarter Way to Bill Observation Services
BellMedEx brings accuracy, speed, and compliance together. Outsource your medical billing to the team that makes getting reimbursed from observation claims a breeze.
Billing Outpatient Observation Hours: How to Count and Report
After selecting the correct billing codes (G0378 for hourly observation and G0379 for direct admissions), the next step is tracking observation time accurately. Your billed hours must always match what’s written in the patient’s medical record.
1). When to Start and Stop the Clock
▶️ Start time: Begin counting when the physician or other qualified provider writes the observation order and the chart shows that care actually started.
⏹️ Stop time: End the count when all observation care is complete.
🚫 Do not count: Any waiting time for a ride, a bed, or nonclinical delays.
Example:
A provider orders observation at 2:00 p.m., and observation care ends at 10:00 p.m. That is 8 hours of observation time.
2). How to Add and Round the Hours
If observation care is interrupted and later resumed, add the time from each segment together. When you have the total time, round it to the nearest full hour. Report that total number of hours as the units on the G0378 line.
Example:
➜ First segment: 3:00 p.m. to 8:15 p.m. (5.25 hours)
➜ Second segment: 9:00 p.m. to 11:10 p.m. (2.10 hours)
Total: 7.35 hours → round to 7 hours, and bill 7 units of G0378.
3). Handling Overnight Observation
When observation continues overnight, keep all hours together on one claim line and use the date when observation began as the service date.
If the patient came as a direct referral from the community, report G0379 on a separate line, and use G0378 for the total observation hours.
Example:
Observation starts at 10:00 p.m. on June 5 and ends at 6:00 a.m. on June 6. Report 8 hours of observation, and use June 5 as the service date.
4). Carving Out Procedures That Include Monitoring
If a procedure or treatment already includes active monitoring as part of its own payment, pause your observation count during that time.
Example:
Observation runs from 8:00 a.m. to 4:00 p.m., but the patient receives chemotherapy from 12:00 p.m. to 2:00 p.m.. Subtract those 2 hours. The remaining 6 hours are reportable observation time.
5). Keep Your Documentation Clear
Make sure the medical record clearly shows:
- The exact start and stop times for observation.
- When a test or procedure occurred and when observation resumed.
- Notes that explain why observation continued.
A simple note such as “Observation paused for chemo from 12:00 p.m. to 2:00 p.m.; resumed at 2:00 p.m.” helps reviewers understand your math and prevents billing questions later.
Length of Medicare Observation: What “long” means

➜ First, set the stage correctly. CMS states that patients are admitted as an inpatient or discharged in less than 24 hours. In rare cases, outpatient observation should go over 48 hours. There is no national bright line, but once you pass 48 hours, many MACs look more closely and expect clear medical necessity in the chart.
Example: If a patient needs IV antibiotics and serial examinations and the team needs until hour 30 to determine inpatient admission, it’s reasonable. If it is after hour 55, the notes must be clear why continued observation was necessary.
➜ Next, recognize that some payors and some MACs have hours in their edits. Some MACs state that observation may be covered for Medicare for up to 72 hours when medically necessary and they instruct non-OPPS providers in the handling of hours in excess of 72 hours, such as reporting it as non-covered on a second observation line. This is a local policy, not a national dictate, so follow your MAC’s written guidance.
➜ Commercial plans may be stricter than Medicare. Some have a 48 hour cap, some may allow no reimbursements above 72 hours. Review the contract, plan policy for observation billing.
Documentation That Supports Observation Billing
Now tie it back to the record. The hours billed must correspond to the record in the patient’s medical record. It must contain at least these items:
- A physician or qualified practitioner order utilizing clear words, i.e. “Place in outpatient observation,” with a specific clock time stated. Avoid the term “admit,” since that implies inpatient.
- Progress notes detailing how continued evaluation or short time treatment is necessary, and why such observation is still appropriate outpatient status.
- Tests and results that support medical need for continued observation care.
Example of order and note:
“3:40 P.M. Place in outpatient observation for chest pain rule out ACS. Serial troponins and ECGs. Reassess hemodynamics and pain control every 2 hours.”
MOON timing
Finally, don’t forget the MOON. The Medicare Outpatient Observation Notice should be delivered to the patient who has been in observation for longer than 24 hours. Deliver the MOON no later than 36 hours after observation starts, or sooner if the patient is discharged, admitted, or transferred before then. Keep proof of delivery in the record.
Example: Observation starts Monday at 10:00 a.m. If the patient is still in observation on Tuesday at 11:00 a.m., the MOON must already be given. If the patient leaves at 8:00 a.m. Tuesday, provide the MOON before discharge.
Observation Billing and Condition Code 44 Basics
Sometimes what you started as inpatient case turns out not to meet inpatient criteria. When that happens, you need to change the patient’s status correctly to outpatient or the bill will not be approved by the payer.
When to use Condition Code 44?
Condition Code 44 (CC44) is to be used if the patient is admitted as inpatient, and Utilization Review (UR) and/or the attending doctor agrees inpatient criteria are not met, and the case is to be converted to outpatient before discharge. The change must happen while the patient is still in the hospital and the rent is billed as outpatient on 13x (hospitals) or 85X (CAHs).
Example: A patient is admitted inpatient for chest pain. At a later time that day, UR and the attending review and agree inpatient criteria are not met, defendant’s status is changed to outpatient with CC44, and the claim is then billed as outpatient.
What must be documented for CC44?
To be valid for billing, the documentation must tell the payer exactly why and when the status changed. This record proves that outpatient billing is correct and compliant.
Document the UR team’s decision, the attending physician’s agreement, the reason for the change and at what time it occurred. Make a clear outpatient order in the chart, alert the patient, and if observation begins, follow the billing rules for observation.
Can we add observation time to cover earlier hours as inpatient?
Observation time begins only when there is a valid outpatient order for observation, and the patient is received in observation. You can not add observation hours to cover prior inpatient time.
OPPS Payment: When is Medicare Paid, and What is Packaged?
The Outpatient Prospective Payment System (OPPS) is how Medicare approves payment for most hospital outpatient services. Under OPPS, Medicare pays hospitals a predetermined amount for each covered outpatient item rather than paying for each item separately.
The claim under this new system will directly affect observation billing, since it determines whether the observation hours will be separately billable or whether they will be packaged with payment for another service, such as an emergency visit or a procedure. Simply stated, you may have coded everything correctly, but it is OPPS rules which control how the claim is paid.
Your Observation Claims Deserve Expert Hands
Outpatient billing errors cost real money. BellMedEx Medical Billing Services handles every rule, code, and OPPS twist so you get paid faster with zero stress.
How does OPPS treat code G0378?
Observation time is a definite entry, but OPPS either qualifies it, or classifies it as to whether it is for separate payment.
Under OPPS, code G0378 is a packaged code. All hours of observation will have to be entered, but it will be left to OPPS to decide whether the claim readily meets the rules set up for composite payments of extended assessment and management.
What must be on the claim for a separate observation payment?
Generally a separate observation payment requires:
- At least 8 hours of billable G0378, and
- A qualifying ED visit, clinic visit, critical care service or direct referral service with G0379.
- If a T-status surgery is given on the same day, or on the previous day, composite payment will not apply. Always report the above services on the same claim, in order for OPPS to apply the proper logic.
Example: You bill 9 hours of G0378 along with an ED visit on one 13X claim. No T-status surgery is present. The claim likely qualifies for the composite payment.
What do we do if the case does not meet the composite rules?
If the required conditions are missing, OPPS will package the observation into another service payment. You should still report all G0378 hours to keep your billing and audit trail complete.
What does “T-status” mean in outpatient billing?
In outpatient billing, Medicare use status indicators to determine payment for each code. A T-status means the procedure is a major surgery or a big treatment that includes the payment for many ancillary services related to that procedure performed on the same day.
Thus, when a T-status procedure is shown on a claim, Medicare’s system will package together other ancillary, minor services such as hours of observation into the major surgical payment.
In other words, T-status means that the surgical payment covers much of the care provided on the same day, including hours of observation.
Example:
A patient has a laparoscopic gallbladder removal in the morning. The procedure is a T-status procedure. The patient is to remain in the hospital until evening for routine recovery. You still record the observation hours on the claim, but Medicare will not pay extra for them because they are already included in the surgery payment.
Knowing what T-status means helps you understand why a claim may not get a separate payment for observation hours, even if you coded everything right. You should still list the observation time for accuracy and audit proof, but expect that OPPS will include that payment in the main surgery.