Cardiology billing is a challenge and even gets more complex with the annual updates in the Medicare Physician Fee Schedule. In 2026, CPT Code 92920 (percutaneous revascularization of a coronary artery, single vessel) has some changes that all cardiology practices need to understand.
CPT code 92920 is used to bill coronary angioplasty services. Healthcare providers must know reimbursement rates for CPT 92920, review physician fee schedules, and correct use of modifiers to maintain a strong revenue cycle for their care practices.
This article explains CPT 92920 in simple terms, including reimbursement outlook for 2026 and documentation requirements for compliance with Medicare and other commercial payers.
What Does CPT 92920 Mean?
CPT 92920 is used for percutaneous revascularization of a coronary artery, single vessel. This means that instead of open-heart surgery, a cardiologist threads a catheter through the skin into the artery and inflates a balloon to reopen the blockage and restore circulation.
If you are a healthcare provider, CPT 92920 is one of the bread-and-butter codes for cardiology billing. You must use this CPT code right since even minor errors can result in claim denials, delay in payment, and external audits.
What Different Payers Pay for CPT 92920?
Average payment for CPT 92920 (percutaneous transluminal coronary angioplasty, single vessel) will vary with each insurance company. According to national averages, however, most insurance companies will pay within a relatively small range. Therefore, there are distinct variations between payers.
| Payer | Average Payment |
| Blue Cross Blue Shield (BCBS) | $747.10 |
| UnitedHealthcare (UHC) | $737.21 |
| Aetna | $707.16 |
| Cigna | $864.99 |
- These figures represent the average “prices” that all major insurers will be charged for the CPT 92920.
- At the low-end, Aetna pays approximately $707 for percutaneous transluminal coronary angioplasty, single vessel.
- In the mid-range, United Health Care and Blue Cross Blue Shield pay approximately $737-$747.
- On the high-end, Cigna pays an average of approximately $865.
As such, on average, Medicare and most commercial payers pay between $700 and $865 for CPT 92920. Although the differences may appear to be minimal, they can have a significant impact when numerous procedures are performed; therefore, it is crucial for providers to understand what their respective payers’ rate will be for CPT 92920.
Modifiers You Will Utilize for CPT 92920
Modifiers are additional codes appended to a CPT code when claiming reimbursement from Medicare or other payers. Modifiers provide additional detail regarding the service, such as whether the service was duplicated, modified, or exceptionally complex. The utilization of modifiers is crucial for the proper reimbursement for cardiovascular procedures such as CPT 92920 (balloon angioplasty) to avoid denials and to ensure correct reimbursement.

Below are the most common modifiers, explained with practical scenarios.
Modifier 76 – Repeat Procedure by the Same Physician
Sometimes, the same cardiologist who performed the first angioplasty must go back and repeat the procedure. This usually happens if the artery narrows or complications arise soon after the initial intervention.
Example: Imagine a patient who has angioplasty in the morning to open the left anterior descending artery. Later that day, the artery closes again, and the same physician performs another angioplasty. Modifier 76 makes it clear this was not a duplicate claim but a repeat procedure by the same doctor.
Modifier 77 – Repeat Procedure by Another Physician
In other cases, a different cardiologist may need to step in. This modifier shows that another physician performed the repeat angioplasty, often due to complications or availability.
Example: A patient develops complications after an angioplasty performed by Dr. A. Dr. B, a colleague, is called in to perform a second angioplasty. Modifier 77 ensures the billing reflects that a different physician carried out the repeat procedure.
Modifier 59 – Distinct Procedural Service
This modifier is used when a separate, distinct service is performed in addition to the angioplasty. It prevents Medicare from bundling two different services into one payment.
Example: A patient receives balloon angioplasty in the left circumflex artery, and during the same session, the cardiologist also places a stent in the right coronary artery. Modifier 59 clarifies that these are distinct services in different arteries, so both are reimbursed properly.
Modifier 52 – Reduced Services
Sometimes an angioplasty is started but cannot be completed, often for patient safety reasons. Modifier 52 indicates that the service was reduced.
Example: A cardiologist begins angioplasty of the right coronary artery, but the patient becomes unstable midway. The procedure is stopped to protect the patient. Modifier 52 shows that only part of the service was performed, ensuring Medicare pays appropriately for the reduced work.
Modifier 22 – Increased Procedural Services
This modifier applies when the angioplasty is unusually complex and requires significantly more time, effort, or resources than normal.
Example: A patient with very twisted coronary anatomy requires prolonged balloon inflation and multiple catheter adjustments. The procedure takes much longer than expected. Modifier 22 documents the extra effort, supporting higher reimbursement.
Anatomical Coronary Artery Modifiers (HCPCS Level II)
These modifiers specify which artery was treated:
- LC – Left Circumflex
- LD – Left Anterior Descending
- RC – Right Coronary
- RI – Ramus Intermedius
They are especially important when more than one artery is treated in the same session.
Example: A patient undergoes angioplasty in both the left anterior descending (LD) and right coronary (RC) arteries. By appending LD and RC modifiers, the claim clearly shows that two distinct arteries were treated. This not only prevents denials but also ensures accurate payment and precise documentation for audits and quality reporting.
Using the right modifiers for CPT 92920 does more than prevent claim denials.
- Modifiers (76, 77, 22, 52, 59) ensure payment reflects repeat procedures, reduced services, or unusually complex angioplasty.
- Clear documentation (e.g., 52 for discontinued angioplasty, 22 for complex anatomy) protects providers during reviews.
- Anatomical modifiers (LC, LD, RC, RI) identify the exact artery treated, improving quality and outcomes data.
- Modifiers like 59 and artery-specific codes distinguish multiple interventions from a single-vessel angioplasty, preventing bundling errors.
Add-On Codes Associated with CPT 92920
When a physician performs percutaneous coronary angioplasty (CPT 92920) in one major artery or branch, additional procedures may be carried out during the same session. The “add-on” codes will document those extra procedures performed at the same time. Add-on codes can never be submitted alone, but must be submitted in conjunction with the primary angioplasty code (92920).
Why Do Add-On Codes Matter?
- Add-on codes represent the total scope of the procedures completed during a single session.
- Add-on codes will provide the provider with proper reimbursement for any additional interventions that were completed.
- Add-on codes will clearly define if a provider has completed a standard angioplasty versus a more complex procedure such as atherectomy, thrombectomy, or advanced imaging.
- Add-on codes will clearly indicate if the procedure was completed in an additional branch of the same artery or a different major vessel (this would require a new primary code).
The Key Add-On Codes for CPT 92920
92921 → Additional branch angioplasty
If the doctor opens up another branch of the same artery during the same session, this code is added to show that extra work.
92925 → Atherectomy with angioplasty
Sometimes plaque needs to be physically removed from the artery. This code (92925) is used when the doctor performs an atherectomy (plaque removal) along with angioplasty in an additional branch.
92973 → Mechanical thrombectomy
If there’s a blood clot blocking the artery, this code is used when the doctor removes it using special mechanical tools.
92974 → Coronary brachytherapy
This is a specialized treatment where radiation is delivered inside the artery to help prevent re-narrowing.
92978 → Intravascular ultrasound (IVUS)
This code 92978 is used when the doctor uses ultrasound imaging inside the artery to get a detailed look at the vessel walls.
92979 → Optical coherence tomography (OCT)
Similar to IVUS, but instead of ultrasound, OCT uses light waves to create very detailed images of the inside of the artery.
Note:
- Codes such as +92921 and +92925 may be used to report up to two additional branches.
- Many of these codes (such as +92921, +92925) are bundled under Medicare’s NCCI guidelines, which means that Medicare may not provide separate payment for these services.
- These add-ons are intended for reporting work performed in additional branches of the same artery. If the provider completes a completely different major vessel, a separate primary code (and not an add-on code) must be reported.
Documentation Required for CPT 92920 (Balloon Angioplasty)
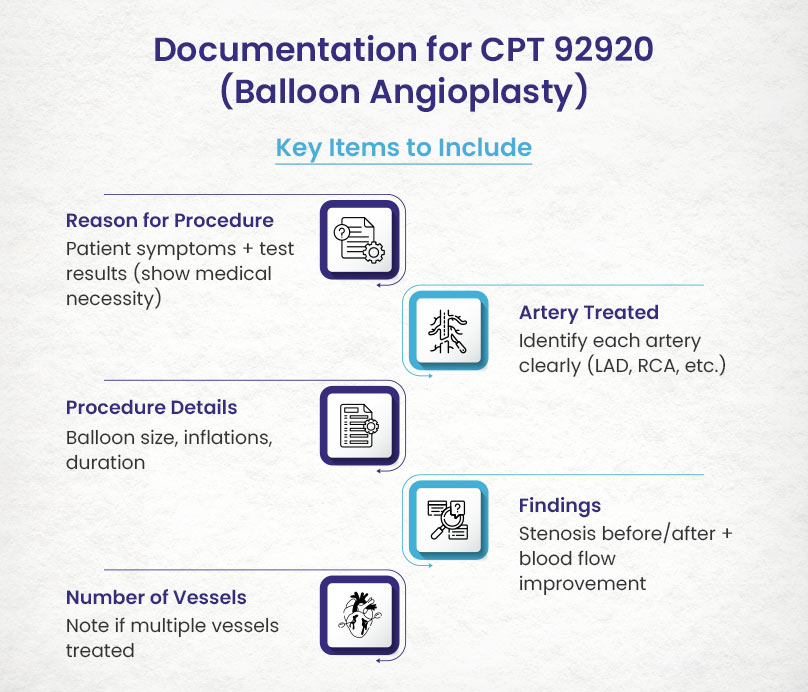
Documentation serves as your protection in the event Medicare or a commercial payer audits your claim. Below is a checklist of items to include when documenting for CPT 92920:
Reason for Performing CPT 92920 (Coronary Angioplasty, Single Vessel)
- Justify why you performed the angioplasty.
- Include patient symptoms (e.g., chest pain, shortness of breath) and test results (e.g., stress tests, angiogram findings).
- You must demonstrate medical necessity. The payer requires evidence that the procedure was not just performed “for fun.”
Which Artery Was Treated
- Identify the artery (e.g., left anterior descending, right coronary artery).
- If you treat more than one artery, identify each one clearly.
- You will want to avoid confusion and demonstrate billing for multiple interventions when applicable.
How the Procedure Was Performed
- List the balloon size, the number of inflations and the duration of inflation.
Example: “3.0 mm balloon inflated twice for 20 seconds each.”
- You should document the technical work completed and support the level of difficulty of the case.
Pre-Procedural and Post-Procedural Findings
- Document the degree of stenosis before (e.g., 90%) and after (e.g., decreased to 10%) the procedure.
- Note any improvement in blood flow.
- You must have to demonstrate the procedure was successful and medically justified.
Number of Vessels Treated
- You want to clearly note in your documentation if you treated more than one vessel.
- Example: “Angioplasty performed in both the LAD and RCA.”
- You have to ensure you receive the proper coding and do not underpay.
Avoiding Denial Traps When Billing CPT 92920
Billing for CPT 92920 (Percutaneous Transluminal Coronary Angioplasty, single vessel) can be challenging. Small errors often lead to reduced reimbursement, denials, or audits. Below are the most common traps and the fixes your team can apply to prevent them.
1). Incorrect Modifier Usage
Missing or misapplied modifiers can cause claims to be down-coded or denied. For example, performing angioplasty in two distinct coronary arteries without modifier 59 may result in payment for only one procedure.
Fix:
- Train staff to recognize when modifiers (e.g., 59, 76, 77) are required.
- Use coding software or claim scrubbers that flag missing or conflicting modifiers.
- Review operative notes carefully to ensure modifiers reflect the actual clinical scenario.
2). Incorrect Site of Service
Payment for 92920 depends on where the procedure is performed (hospital outpatient, ASC, physician office). Submitting the wrong site of service can lead to denial, incorrect payment, or later audit.
Fix:
- Verify the place of service before claim submission.
- Align billing with the facility records to ensure consistency.
- Conduct periodic audits of claims to catch mismatches early.
3). Bundled Services Billed Separately
Certain services, such as diagnostic angiography performed during angioplasty, are bundled into the payment for 92920. If billed separately, the secondary service will be denied, though the primary procedure is usually still reimbursed.
Fix:
- Educate billing staff on bundling rules for cardiovascular procedures.
- Use coding references (e.g., Medicare guidelines, payer manuals) to confirm which services are bundled.
FAQ’S
What does the CPT Code 92920 represent?
The CPT Code 92920 represents Percutaneous Transluminal Coronary Angioplasty (PTCA) that has been done in a single coronary artery or branch; 92920 is a billing code that identifies the procedure for insurance companies to pay for.
When would you report CPT 92920?
You would report CPT 92920 when Percutaneous Transluminal Coronary Angioplasty (PTCA) is being performed without the use of a stent and you are working in only one major coronary artery or branch; if you perform PTCA in additional branches you will need to report CPT 92921 as well as an add-on to your CPT 92920.
What is the typical national reimbursement amount for CPT 92920?
The 2026 national average reimbursement amounts for CPT 92920 are as follows:
- Blue Cross Blue Shield (BCBS): $747.10
- United Healthcare (UHC): $737.21
- Aetna: $707.16
- Cigna: $864.99
Medicare and all other commercial insurers pay between $700-$865 on average for this type of procedure.
What are some common types of billing errors made with CPT 92920?
Common billing error examples include missing or incorrectly placed modifiers, wrong site of service (for example, billing as an office visit instead of a hospital visit), unbundling services (billing for angiography as a separate procedure from angioplasty when they are typically performed as a bundle).
Does CPT 92920 include diagnostic angiography?
No, CPT 92920 only includes the performance of angioplasty and does not include diagnostic angiography that may be required to determine where to place the balloon catheter for the PTCA procedure. If medical necessity exists, providers may submit a separate claim for diagnostic angiography that was performed prior to the PTCA procedure; however, if the diagnostic angiography is performed as part of the PTCA procedure, then it is considered a bundled component and cannot be submitted separately.