The 2026 CMS emergency department updates require immediate attention from the billing teams. And action, too. If you and your staff still rely on outdated CMS emergency room billing guidelines, you are risking automated claim rejections, severe audit penalties, and massive revenue leaks.
Understanding and executing these new CMS mandates is no longer optional. It is critical for your facility’s financial survival in 2026 and onward.
Want to know what’s included in the updated CMS guidelines for emergency departments?
Keep reading as we discuss the dual-billing foundation, new conversion factor rates, telehealth parameters, critical hospital mandates, and emergency psychiatric rules.
The Dual Billing Pathway in Emergency Room Billing: Professional vs. Facility Billing
Before going into the details of CMS 2026 guidelines, you must be aware of a fundamental rule of emergency room billing.
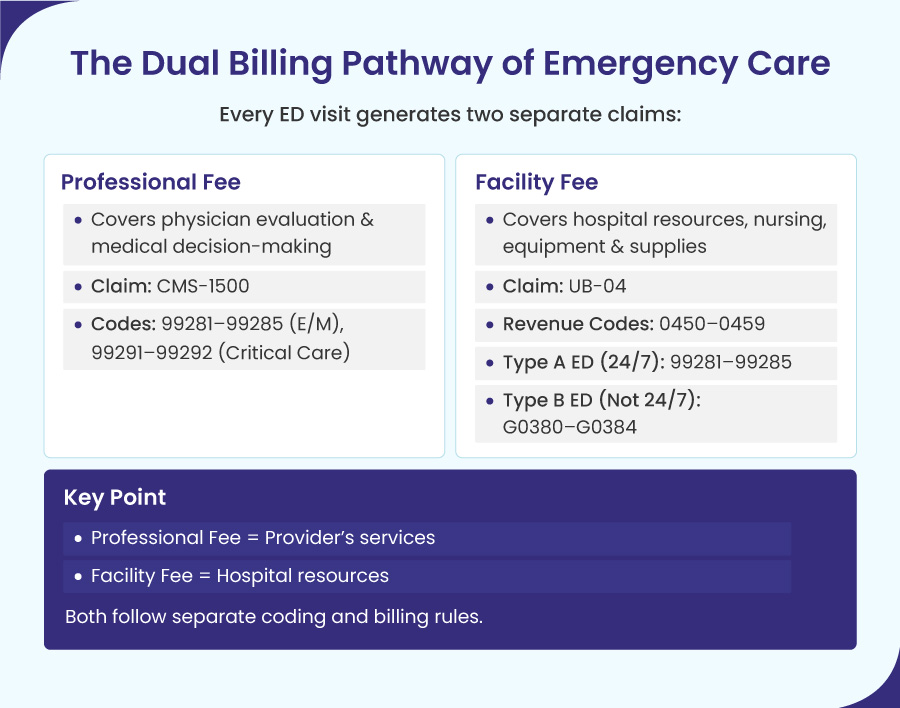
Every patient encounter in the emergency department begins with two separate billing pathways. These pathways map to two completely different cost structures and follow distinct coding rules. Mixing them is a serious mistake that can torment your revenue flow.
The Professional Fee: ED E/M Codes 99281-99285 and Critical Care Billing
The professional fee is charged for the provider’s cognitive work and diagnostic skills. The provider reports this service on a standard CMS-1500 claim form with place of service code 23 (POS 23). The code selection depends entirely on the official evaluation and management (E/M) guidelines. The specific CPT codes used for professional fees are divided by the complexity of the patient’s condition.
These are:
- 99281 (Level 1): Minimal complexity, like a minor wound check, simple bandage change.
- 99282 (Level 2): Low complexity evaluation for stable or self-limited conditions.
- 99283 (Level 3): Moderate complexity evaluation for stable acute illnesses.
- 99284 (Level 4): High complexity evaluation for acute illnesses with systemic symptoms.
- 99285 (Level 5): Highest complexity evaluation reserved for severe, life-threatening injuries or illnesses.
- 99291 & 99292 (Critical Care): Used when a provider must spend continuous, face-to-face time treating a patient whose illness or injury puts them at immediate risk of death. 99291 reports the first 30–74 minutes of critical‑care time, and 99292 is billed for each additional 30 minutes.
The Facility Fee: Hospital Facility Billing Under OPPS
The facility fee covers the institutional costs of the hospital. In simple words, it covers the costs of the physical space, nursing workforce, specialized equipment, and disposable medical supplies. You bill this service on a UB-04 institutional claim form under the Outpatient Prospective Payment System (OPPS).
The Facility Billing Code Structure for Emergency Departments
To get a facility claim paid, the hospital must put two types of codes on the UB-04 form: a 4-digit department code and an acuity level code.
1). Emergency Room Revenue Codes (The 045X Series)
This code series specifies exactly which room inside the hospital was used:
- 0450: General Emergency Room
- 0451: EMTALA Emergency Screening (The baseline legal exam)
- 0452: ER Care beyond the initial screening
- 0456: Urgent Care clinic inside the hospital
- 0459: Special or unique emergency rooms
2). ED Levels of Service (Type A vs. Type B Emergency Departments)
While these numbers look like the doctor’s codes (already mentioned under professional pathway), the facility chooses them based on nurse time and supplies used, not the doctor’s diagnosis.
Type A Emergency Departments (Open 24/7): These emergency departments classify visits into five levels according to resource intensity:
- 99281 (Level 1): Lowest resource intensity (e.g., basic triage assessments, simple bandage applications).
- 99282 (Level 2): Low resource intensity (e.g., minor interventions, single medication administration, or simple dressing changes).
- 99283 (Level 3): Moderate resource intensity (e.g., specialized localized care, basic lab draws, or a single diagnostic X-ray).
- 99284 (Level 4): High resource intensity (e.g., prolonged nursing care, multiple IV medications, or complex multi-system diagnostic testing).
- 99285 (Level 5): Maximum resource intensity (e.g., continuous nursing observation, trauma bay allocation, or advanced stabilization protocols).
Type B Emergency Departments (Dedicated ERs NOT open 24/7): CMS forbids these part-time facilities from using regular CPT codes. They must use these specific G-codes instead:
- G0380 to G0384: These HCPCS codes represent Levels 1 through 5 facility Evaluation and Management (E/M) care.
For facility reporting of critical‑care encounters, hospitals continue to use revenue code 0450 with an appropriate acuity level. However, the professional CPT codes 99291/99292 are billed separately on the CMS‑1500.
The Core CMS E/M Framework: Medical Decision Making in the Emergency Department
To code accurately under CMS guidelines, you must discard the rules used in traditional doctor offices. In a standard clinic, providers can select a billing level based on either time or medical decision-making.
In the emergency department, time does not matter.
For standard emergency codes 99282 through 99285, you cannot use the clock to determine your code level. A patient could occupy an emergency bed for six hours. But if the medical intervention is simple, the billing level stays low. You must select the code based entirely on the complexity of Medical Decision Making.
CMS measures this complexity using three specific components:
- The number and complexity of problems addressed: This tracks how severe the illness or injury is during the visit.
- The amount and complexity of data reviewed: This counts the lab tests, imaging studies, and old medical records that the provider must analyze.
- The risk of complications or patient morbidity: This measures how dangerous the diagnostic choices or treatment options are to the patient’s life.
To qualify for a specific code level between 99282 and 99285, your provider’s chart notes must support medical necessity and hit the target requirements for at least two of these three components. This framework scales across the following distinct levels:
- 99281 (Level 1): The only exception to the rule. This level covers minor issues that do not require a doctor’s physical presence (e.g., a nurse checking a small scrape). It does not use the decision-making components listed above.
- 99282 (Level 2) to 99284 (Level 4): Covers straightforward, low, and moderate medical situations requiring a physician’s evaluation.
2026 Medicare Reimbursement for Emergency Department Services Explained
The Centers for Medicare & Medicaid Services (CMS) has made major changes to the Physician Fee Schedule 2026, which directly affect emergency medicine revenue. To manage these changes, it’s important to understand how the new conversion factors work with efficiency and practice expense adjustments.
The 2026 Medicare Conversion Factor Update
The 2026 Medicare conversion factor for physicians not in Advanced Alternative Payment Models (APMs) is $33.4009, a 3.26% increase over the previous year.
This 3.26% increase is built on three distinct regulatory mechanisms:
- A 0.25% statutory increase under the Medicare Access and CHIP Reauthorization Act (MACRA).
- A 0.49% positive budget neutrality adjustment.
- A 2.5% one-time payment boost passed under federal legislation.
For clinicians qualifying under Advanced Alternative Payment Models (APMs), the conversion factor receives an additional 0.75% bump, resulting in a 3.77% increase.
The 2.5% Efficiency Adjustment and Its Impact on ED Procedure Billing
While the conversion factor went up, CMS offset some of those gains by finalizing a -2.5% efficiency adjustment. This reduction stems from a comprehensive five-year review of Medicare Economic Index productivity data. This cut slashes Work Relative Value Units (wRVUs) for non-time-based services and impacts intraservice physician time.
There is a vital piece of good news for emergency medicine. CMS explicitly excluded standard Emergency Department Evaluation and Management (E/M) codes, Observation codes, and Critical Care codes from this -2.5% efficiency adjustment.
But this exclusion does not apply to procedures. All surgical or medical procedures done in the emergency department will face the full -2.5% wRVU cut. This affects common ED interventions such as:
- Laceration repairs and complex wound closures.
- Intubations and central line placements.
- Fracture care and joint reductions.
- Splint and cast applications.
Practice Expense Rebalancing for Facility-Based Emergency Medicine
The third component of the 2026 financial reality is the rebalancing of the Practice Expense (PE) portion of RVUs. CMS changed its methodology for allocating indirect practice expenses, which represent the administrative overhead of operating a clinical practice.
CMS’s changes to indirect practice-expense RVUs will lower payments for facility-based services by about 7% and raise payments for non-facility services by about 4%. Because of this, emergency department E/M codes stay about the same, while critical care services drop by around 3% and observation services by 5 to 7%.
This rebalancing heavily disadvantages facility-based services. Because emergency rooms operate entirely within institutional facility settings, emergency medicine groups will see a notable reduction in their PE RVUs.
The data shows a disparate impact across specific ED care models:
- Standard ED E/M Visits (99281-99285): The combination of the conversion factor increase and the PE reduction results in a net neutral or slightly positive revenue shift of 0% to +1%.
- Critical Care Services: Due to the severity of the PE adjustments, critical care reimbursement faces an estimated 3% reduction.
- Observation Services: Hospital-based observation codes experience the steepest decline, with projected revenue drops between 5% and 7%.
| Specialty Service Category | wRVU Efficiency Adjustment | PE RVU Shift | Estimated Net Revenue Impact |
| Standard ED E/M (99281-99285) | Exempt (0% cut) | Negative Facility Shift | 0% to +1% (Flat) |
| ED Procedures (Surgical/Invasive) | Full 2.5% Reduction | Negative Facility Shift | Modest Net Decrease |
| Critical Care Services | Exempt (0% cut) | Major Facility Drop | -3% Reduction |
| Observation Services | Exempt (0% cut) | Severe Facility Drop | -5% to -7% Reduction |
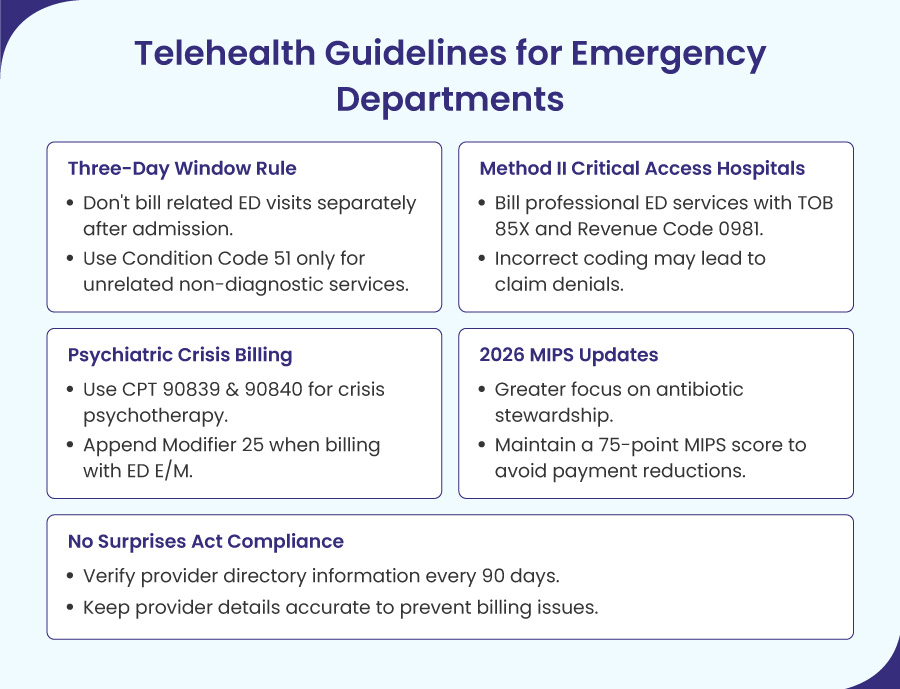
Telehealth Guidelines for Emergency Departments
Under the CY 2026 guidelines outlined in CMS Change Request 14315, Medicare has officially streamlined its Telehealth Services List by completely removing the old distinction between provisional and permanent services.
Moving forward, CMS limits its review to one core question: can the service be successfully furnished using an interactive, two-way audio-video telecommunications system?
This policy change helps make the evaluation process more stable in complex care settings. From 2026, the new framework allows supervising physicians to oversee required services using real-time audio and video technology, but not audio-only connections.
In teaching settings, CMS has also adopted a permanent policy that allows virtual direct supervision during three-way telehealth visits with the patient, resident, and teaching physician, all in different locations.
Emergency departments should make sure their clinical oversight processes meet these new criteria and regularly check the CMS list for approved interactive tools.
Medicare’s Three-Day Payment Window Bundling and Condition Code 51
One of the most complex areas of compliance occurs when an outpatient emergency department visit directly precedes an inpatient hospital admission. Under the Medicare Three-Day Payment Window policy, improper billing across these two settings will trigger immediate claim denials.
The Mechanics of the Three-Day Payment Window for ED Claims
The three-day payment window applies to all hospitals operating under the Inpatient Prospective Payment System (IPPS). For non-IPPS hospitals, a one-day window applies.
The policy states that if a hospital or an entity owned or operated by the same health system provides outpatient services to a patient within three days before an inpatient admission, those outpatient services must be included in the inpatient claim for billing.
This bundling rule splits cleanly between technical and professional billing components:
1). The Technical Component (Facility Fees)
The hospital cannot submit a separate outpatient claim (Type of Bill 13X) for the ED facility fee, diagnostic labs, or imaging performed during those three days.
The technical costs of all diagnostic and related non-diagnostic outpatient services must be rolled into the final inpatient claim (Type of Bill 11X).
2). The Professional Component (Physician Fees)
The professional fees for the emergency room physician’s evaluation and management work are billed separately on a standard CMS-1500 form.
However, the physician must use the appropriate inpatient place-of-service code if the outpatient work was inextricably linked to the subsequent admission.
Preserving Separate Payments with Condition Code 51
There is a critical regulatory exception to this automatic bundling rule. If a patient receives non-diagnostic outpatient services in the emergency department that are entirely unrelated and clinically distinct from the reason they are subsequently admitted as an inpatient, the hospital can preserve its separate outpatient facility payment.
To bypass the automatic three-day bundling edit, the hospital must apply Condition Code 51 to the outpatient facility claim.
CMS Compliance Requirement
Condition Code 51 is a special label used to say: “The emergency room visit and the hospital stay were for two completely different medical problems.”
To use it, the doctor’s notes must clearly prove that the ER visit had absolutely nothing to do with why the patient was admitted to the hospital.
Diagnostic services, such as lab tests and X-rays, can never use Condition Code 51; they are always bundled if they occur within the three-day window, regardless of the clinical rationale.
Example of an ED Billing Scenario
Suppose a patient arrives at an integrated health system’s emergency department on Monday after a slip-and-fall. The ED physician diagnoses a non-displaced wrist fracture, applies a splint, and discharges the patient. This is a non-diagnostic outpatient service.
On Wednesday afternoon, unfortunately, the same patient suffered sudden, severe abdominal pain and was admitted to the same hospital as an inpatient for an emergency appendectomy.
Because the Monday emergency department visit for a wrist fracture is completely unrelated to the Wednesday inpatient admission for appendicitis, the hospital should not bundle the encounters.
The billing team must submit the Monday ED claim separately by appending Condition Code 51. This tells the Medicare Administrative Contractor (MAC) that the services are distinct, ensuring the hospital gets paid for the ED visit as well as the inpatient surgery.
The Method II Critical Access Hospital ED Billing Mandate
Starting April 24, 2026, the Centers for Medicare & Medicaid Services (CMS) tightened the rules for how rural hospitals known as Method II Critical Access Hospitals get paid for emergency room doctor services.
They issued a new manual update (Change Request 14342) to prevent these hospitals from accidentally or intentionally billing for regular clinic visits as emergency room visits, which was leading to widespread overbilling.
The OIG Audit Catalyst
A Method II Critical Access Hospital is a small, rural facility where physicians have formally reassigned their billing rights to the hospital. This allows the CAH to submit a single, combined claim covering both the technical facility operations and the professional medical services.
CMS issued Change Request 14342 following a scathing Office of Inspector General (OIG) audit. The OIG discovered systemic overpayments across the country. Method II hospitals were routinely billing Medicare for professional emergency department procedures when the services were actually performed in standard outpatient clinics, non-emergent urgent care wings, or regular physician offices.
The OIG and CMS reiterated a fundamental rule that billing for professional emergency department services is illegal if the physical site of service is anywhere other than an official, designated emergency department.
The Strict 2026 CAH Emergency Department Billing Parameters
To eliminate these overpayments, CMS added Section 250.18 to Chapter 4 of the Medicare Claims Processing Manual. This section mandates that Medicare Administrative Contractors only reimburse professional ED procedures under the Method II structure if the facility adheres to a rigid billing protocol.
If your rural health network operates a Method II CAH, your billing team must configure your clearinghouse to enforce the following data combinations:
- Form Type: The claim must be submitted electronically in institutional formats matching the standard UB-04 hard copy.
- Type of Bill (TOB): The facility must use Type of Bill (TOB) 85X.
- Revenue Code: All professional emergency services must be tied to Revenue Code 0981 (Professional Fees – Emergency Room).
- CPT Procedure Codes: Revenue Code 0981 must only be paired with standard emergency department evaluation and management codes 99281, 99282, 99283, 99284, or 99285.
If a billing team attempts to clear professional ED codes using standard clinic revenue codes like 0510 or 0520, or if they attempt to submit these services under a non-ED revenue code, the MAC system will automatically reject the claim.
Billing for Psychiatric Crises in the Emergency Department
Nowadays, emergency departments are seeing more patients with acute behavioral health crises than ever before. CMS has updated its provider manual to clarify billing and documentation requirements for these complex cases.
Coding Psychotherapy for Crisis (CPT 90839 and 90840)
When a patient arrives at the emergency department in severe distress from life-threatening psychological issues, clinicians should use Psychotherapy for Crisis codes instead of standard psychiatric codes.
These cases often involve active suicidal thoughts, acute psychosis, or serious drug-induced delirium.
The crisis coding structure relies on two time-based codes:
- CPT Code 90839: Psychotherapy for crisis; first 60 minutes of continuous, direct face-to-face clinician time.
- CPT Code 90840: Each additional 30 minutes of crisis psychotherapy (reported as an add-on code alongside 90839).
NCCI Bundling Edits and Modifier 25 Rules for ED E/M Codes
A frequent compliance error occurs when an emergency department physician or a consulting psychiatrist performs both a medical evaluation and a crisis psychotherapy session during the same ED encounter.
Under National Correct Coding Initiative (NCCI) edits, Medicare explicitly permits a provider to report both an E/M service (99281-99285) and crisis psychotherapy (90839-90840) on the same date of service. However, they must meet the strict three-point criteria explained below.
1). Separate and Identifiable Work
The medical assessment and the psychotherapy must be significant, distinct, and separately identifiable. A separate psychiatric diagnosis code is not required to justify billing both services.
2). The Modifier 25 Mandate
The billing team must append Modifier 25 to the emergency department E/M code. This tells the payer that the medical evaluation was entirely separate from the crisis psychotherapy session.
3). Strict Time Partitioning
Time is the ultimate audit vulnerability here. Any time the clinician spends performing standard medical E/M work cannot be counted toward the time requirement for the crisis codes.
ED Documentation Requirements for Crisis Billing
In the clinical notes, the doctor must split their time into exact numbers. They must show exactly how many minutes they spent on medical work (like checking labs or vitals) and exactly how many minutes they spent on crisis therapy.
If an auditor sees overlapping time descriptions, the entire psychotherapy payment will be recouped.
2026 MIPS Quality Measure Overhauls for Emergency Medicine
The Merit-based Incentive Payment System (MIPS) directly influences a practice’s future Medicare reimbursement. For 2026, CMS enacted major modifications to the Emergency Medicine MIPS Value Pathway (MVP), shifting the reporting burden away from social screening and heavily toward antibiotic stewardship.
The Removal of Standalone SDOH Measures
In a surprising regulatory pivot, CMS officially removed two primary social tracking metrics from the Emergency Medicine MIPS category list. These are:
- QID487: Screening for Social Drivers of Health (SDOH).
- QID498: Connection to Community Advisor.
Even though this requirement has been removed, social factors still matter. Clinicians should continue to document social challenges using ICD-10-CM code categories Z55 through Z65.
This information is still important when figuring out the “Risk of Complications” in standard Medical Decision Making (MDM) E/M guidelines. But now, providers do not have to track and report these screenings separately for MIPS quality points.
Modified Antibiotic Stewardship Metrics
To combat the rampant overprescription of antibiotics in emergency settings, CMS heavily modified three core clinical quality measures. Emergency medicine groups must adjust their electronic health record (EHR) smart-texts to track these updated metrics:
- HCPR24 (Appropriate Utilization of Vancomycin for Cellulitis): This rule pushes doctors not to use heavy-duty, expensive IV antibiotics like vancomycin for minor skin infections when a simple, targeted pill would work just as well and be safer for the patient.
- QID065 (Appropriate Treatment for Upper Respiratory Infection): This metric tracks the percentage of patients diagnosed with acute URIs who were correctly not prescribed antibiotic medications.
- QID116 (Avoidance of Antibiotic Treatment for Acute Bronchitis/Bronchiolitis): This measure enforces strict compliance guidelines against prescribing antibiotics for viral bronchial inflammation.
The 75-Point MIPS Penalty Threshold
CMS finalized that the overall MIPS performance threshold will remain locked at a rigid 75 points. This threshold is fixed through the 2028 performance year. Because the baseline is high, an emergency medicine group cannot afford to drop points.
Failing to meet or exceed the 75-point score will result in a negative payment adjustment that reduces your Medicare Part B professional payments beginning two years later in the associated payment year.
No Surprises Act Directory Compliance for Emergency Departments
Most people think the ‘No Surprises Act’ is just about surprise medical bills and cost estimates. But there is a hidden risk for emergency rooms involving the need to keep their doctor lists accurate for insurance companies.
If a hospital’s public directory information is incorrect, it can cause major billing and compliance headaches.
The 90-Day Verification Mandate
According to federal law, every hospital and doctor’s group must verify that their public contact information, including their address, phone number, and which insurance plans they accept, is 100% correct every 90 days.
This verification must confirm:
- The exact physical addresses of all active practice locations.
- The precise roster of practicing providers currently taking patients at those locations.
- The exact network participation status across all contracted commercial health plans.
Maintaining Directory Accuracy
Health plans need to check each provider’s directory information at least every 90 days. Providers should let plans know right away if their practice location, phone number, or network status changes.
If an insurance company can’t verify a provider’s information, they temporarily remove or flag that provider’s name in their provider search tool.
To keep getting paid on time and avoid these issues, the provider’s team should set a recurring 90-day calendar reminder to update and confirm directory information before the deadline.
Actionable ED Revenue Cycle Checklist for 2026 Compliance
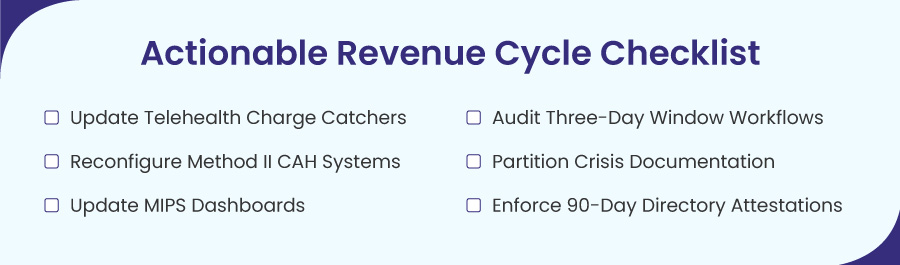
To ensure your emergency department complies with the new 2026 rules and avoids late reimbursements, you must follow these operational steps.
✅ Update Telehealth Charge Catchers
A strict review of your EHR charge-capture rules is necessary. It helps ensure that telehealth services are in line with the CMS standards. The old distinction between provisional and permanent services is gone. All virtual visits now require a real-time, two-way audio-video connection.
Additionally, verify that your virtual direct supervision workflows for clinicians and teaching physicians meet these permanent audio-visual mandates.
✅ Audit Three-Day Window Workflows
Train hospital billing staff to audit all inpatient admissions for preceding ED visits within a three-day window to ensure Condition Code 51 is applied only to completely unrelated non-diagnostic encounters.
✅ Reconfigure Method II CAH Systems
For rural facilities, cross-reference all claims to ensure professional ED procedures are clear on Type of Bill 85X with Revenue Code 0981.
✅ Partition Crisis Documentation
Review psychiatric crisis templates to ensure physicians explicitly separate medical E/M time from crisis psychotherapy minutes (90839-90840).
✅ Update MIPS Dashboards
Work with your EHR vendor to delete the removed measures QID487/QID498 and upload the newly modified antibiotic stewardship parameters.
✅ Enforce 90-Day Directory Attestations
Establish an automated calendar alert to submit provider roster verifications to all major payers every 75 days to completely avoid the No Surprises Act directory removal penalty.



