Medicare billing can be confusing for psychiatry and behavioral health practices. One of the most confusing policies is incident-to billing. Most providers have heard of it, but few understand the details of how it works.
When used properly, incident-to allows for 100% physician payment for follow-up care provided by nurse practitioners, physician assistants, or other licensed mental health provider staff. Additionally, it allows psychiatrists to concentrate on more complex cases while giving patients more timely access to psychotherapy and counseling visits.
This article will explain what incident-to billing means for mental health care, why it matters, who may bill incident-to, and the most recent updates for 2025.
What is Incident-to Billing in Mental Health?
Incident-to billing is a process for a clinic to bill at the higher physician rate, when the care is actually provided by someone else on the treatment team.
Here is how it works:
First, the supervising clinician, usually a psychiatrist, sees the patient for the first time, and develops a plan of care. Then, another qualified member of the treatment team (a nurse practitioner, physician assistant, licensed therapist) provides care for the patient, utilizing the original plan. Billing occurs under the supervising clinician’s name and not under the name of the individual who performed the service in place of the supervising clinician.
Medicare pays successfully as if the visit was done by the supervising clinician. The clinic reimbursement is 100% of the normal rate, as opposed to the reduced rate paid if the nurse practitioner or PA billed under their name.
Some Key Rules
➠ The supervising clinician must see the patient first to start the plan. If a patient comes back for a new issue later, the clinician with supervision must re-review the patient and update the plan, prior to the next visit by a team member.
➠ The person providing the service must possess the state education/credential requirements, and federal education/credential requirements in order to bill for services to Medicare patients.
➠ The supervising clinician must remain involved during care. No in-person supervision is required for most mental health services anymore, but, the clinician must be accessible and overseeing the basic care.
➠ This only applies to outpatient care setting, not hospital or nursing home care settings.
Importance of Incident-to Billing for Mental Health Specialties

Operating a mental health practice means far more than providing patient care. You schedule long visits, organize frequent check-ins, supervise medication adjustments, document activities, and receive a stream of refill requests. You’re full in the schedule, your team is busy, and you’re also running the business side.
Incident-to billing can be a huge help for mental health and psychiatric specialties.
When appropriately used, it allows you to delegate routine follow-ups to qualified team members while keeping your oversight in place. You are able to spend your time on more complex cases, increase patient access, and get paid at the full physician rate.
Here’s why, incident-to billing is important for mental health specialists:
✅ Stability in clinic reimbursements
Nurse practitioners or physician assistants who bill under their own NPI are reimbursed by Medicare at 85% of the physician fee schedule rate. When the visit is incident-to, billed under the physician’s NPI, Medicare reimburses at 100%. This fifteen-point differential provides for the costs of staffing and follow-up work across the year.
✅ Better practice access with team follow-ups
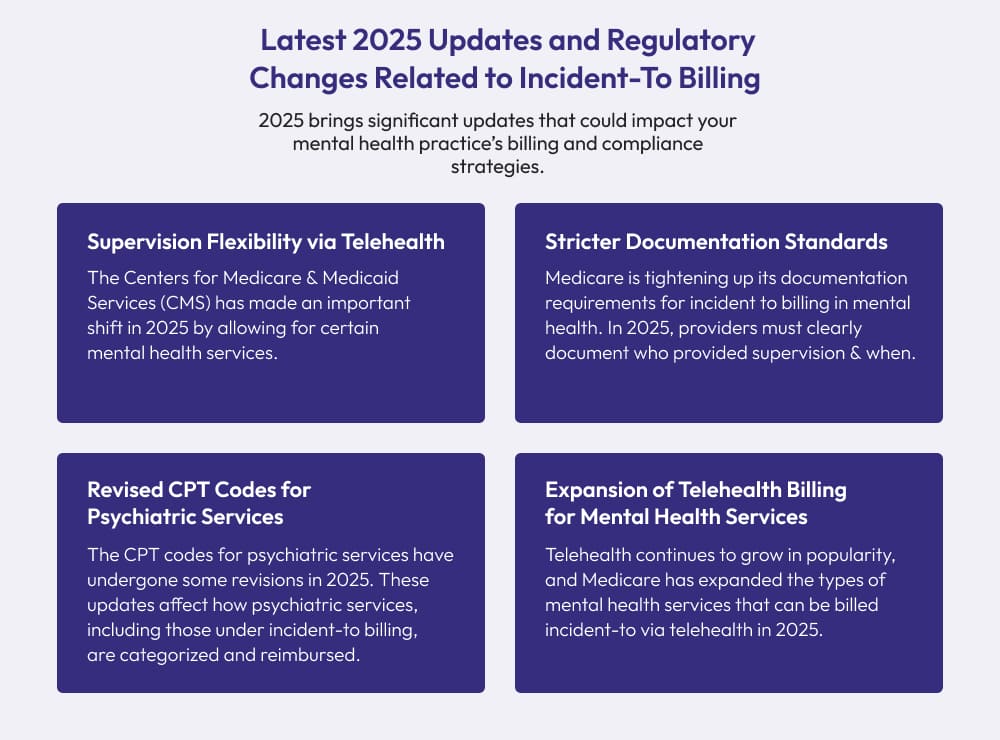
The supervising clinician develops the plan to begin with and continues to supervise this plan. Qualified team members complete routine follow-ups within this plan. By doing this, appointment times become free, and waits decrease, without any violation of Medicare stipulations. Starting in 2024, Medicare made all this easier by formally allowing the use of general supervision in relation to behavioral health services delivered incident-to, therefore providing an opportunity for clinics to be more flexible with scheduling while still maintaining supervision.
✅ Improved day-to-day operations
Using the team to provide routine visits keeps clinics moving in the schedule, able to accommodate same-day requests. Medicare Policy now permits general supervision for behavioral health incident-to services, which conceptualizes the workflow, because the supervising clinician may supervise the delivery of care, without being in the room for each follow-up.
✅ Pragmatic solution for sustainability
Many mental health clinics have a small margin to operate within. Collecting full physicians rate allows for continued hours versus curtailing hours. This point draws directly from Medicare’s payment policy for physicians versus advanced practice clinicians.
Eligibility Criteria for Incident-To Billing in Mental Health Clinics
Not all psychiatry visits are eligible for incident-to billing. Medicare has strict parameters. These parameters are very important in psychiatry and therapy environments.
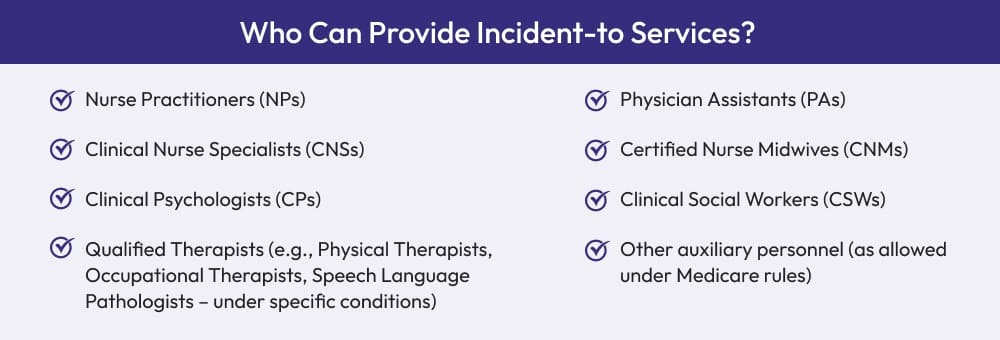
1). Who can provide the service
Qualified team members can conduct the office visit as long as it stays within the treatment plan that the billing clinician initiated. Under Medicare, these team members are called auxiliary personnel. They can be employees or contracted staff and must work within state scope and your practice’s expense. This group includes nurse practitioners, physician assistants, psychologists, social workers, and other licensed clinicians when allowed by state law and every incident-to guideline is followed.
NOTE: As of January 1, 2024, MFTs and MHCs can enroll and bill for psychotherapy to Medicare on their own. Medicare will pay these services at 75% of the clinical psychologist rate. You can continue to use incident-to billed under a physician or other eligible billing practitioner when permissible and appropriate.
2). Who must supervise and bill
The claim is billed under a Medicare-recognized billing practitioner. In behavioral health services, a psychiatrist is often the billing practitioner. A physician in primary care, clinical psychologist, NP, PA, CNS, or CNM can also be the billing provider, if permitted for that service and in that setting. If the billing practitioner is a physician, payment is 100% of the established payment rates. If an NP or PA bills (not incident-to the physician), payment will be 85% of the established rates.
3). What degree of supervision is required
In the case of mental health, many team members providing “incident-to” activities can be done under general supervision. General supervision means that the billing clinician is directing the care and is available, if needed, but does not need to be present in the patient encounter in person, or present in the room or working in the office at that time. Medicare implemented this option for behavioral health under its regulation at 42 CFR 410.26.
However, not every service has general supervision. Some services still require direct supervision. Direct supervision could be present in person, or by real-time audio-video communication under the “virtual direct” rules, which Medicare has extended until December 31, 2025.
4). The plan comes first
The billing practitioner sees the patient first. The diagnosis and treatment plan is initiated by the billing practitioner. Follow-up visits that stay with that plan can be incident-to. If a different problem or reason for visit emerges, the billing practitioner must assess and revise the plan, and document the plan prior to the next incident-to visit. Link the treatment plan for continuity of care each time.
5). The place of service matters
You can use incident-to in a clinic or office. You cannot use incident-to in a hospital or skilled nursing facility under Part B. In hospitals or skilled nursing facilities, the care is paid under different rules and payment bundles. Those settings have their own Part B directions and rules, thus the office-style incident-to does not apply.
Outsource Incident-to Billing to BellMedEx
Thin margins are real in mental health. BellMedEx Medical Billing Services Company helps you maximize revenue so your psychiatry and therapy practice can grow, not shrink.
Incident-To Billing vs. Supervisory Billing in Mental Health
Think of incident-to and supervisory billing as cousins, not twins. While both are forms of billing that involve supervision, they are used in different contexts, and understanding the distinction is key to getting paid properly in your mental health practice.
| Aspect | Incident-To Billing | Supervisory Billing |
|---|---|---|
| Definition | A Medicare rule: services are provided by licensed auxiliary staff (NPs, PAs, psychologists, LCSWs, etc.) under a supervising clinician’s treatment plan. | A payer or state-level practice: therapy provided by a pre-licensed therapist under oversight of a licensed professional for training/licensure. |
| Who Provides the Service | Auxiliary personnel who are licensed and qualified under state law (e.g., NP, PA, clinical psychologist, LCSW). | Pre-licensed therapists, associates, or trainees working toward full licensure. |
| Who Bills | The supervising, Medicare-recognized provider (often a physician). If billed under physician NPI, payment is 100%; if under NP/PA, payment is 85%. | The clinic bills according to the commercial plan or Medicaid policy. Medicare Part B generally does not cover pre-licensed services in private practice. |
| Supervision Required | Behavioral health services by auxiliary personnel can be under general supervision (billing clinician guides care, not required in the room). Some other services require direct or “virtual direct” supervision. | Licensed clinician provides clinical supervision for licensure. Oversight is for training purposes, not tied to Medicare’s incident-to rules. |
| Common Services | Medication management, follow-up visits, psychotherapy or counseling by licensed staff, brief nurse visits (e.g., 99211). | Psychotherapy or counseling provided by pre-licensed associates or trainees (coverage varies by payer, not by Medicare). |
| Billing Rate | Paid at the supervising physician’s full rate (100%) if billed under physician. Paid at 85% if billed directly by NP/PA. | Typically reimbursed at lower rates, depending on payer. Medicare Part B does not reimburse pre-licensed staff in private practice. |
| Documentation | Must show supervising clinician started the plan, remains involved, and that follow-ups stayed within that plan. | Must show licensed supervisor oversight for training and any payer-required supervision notes. |
| Medicare Eligibility | Strictly defined under 42 CFR 410.26; only covered in office or clinic, not hospital or SNF Part B. | Not a Medicare Part B benefit in private practice. May be allowed by some commercial insurers or Medicaid programs. |
| Flexibility | Narrower rules, but higher pay when criteria are met. | More flexible in terms of who can see patients, but usually lower pay and not recognized by Medicare. |
Incident-To Billing FAQs for Mental Health
Can a nurse practitioner supervise incident-to services?
Yes, under certain conditions. Nurse practitioners are permitted to supervise the care and bill under their own name if all relevant state laws and Medicare rules are followed. If that is the case, then they would get 85% of the physician rate. If the caring is billed under the physician’s name, then it would be full 100%.
What if the supervising provider is not present in the office?
For many mental health services, the supervising provider does not even need to be present. Medicare allows general supervision, which means as long as the supervising provider is providing supervision and is available but not actually on site, the service is billable. For some services which still require direct supervision, Medicare has allowed “virtual direct” supervision using live video until at least the end of 2025.
Are there exceptions for rural or underserved areas?
Yes. The same virtual direct supervision rule applies to rural and underserved clinics, and the supervising provider can connect by live video rather than physically residing in the building.
Can a social worker or associate therapist bill incident-to?
No, unlicensed associates are not eligible to bill Medicare, even if a supervising provider is conducting the supervision. Licensed social workers and psychologists do not need incident-to their supervision — they can bill Medicare directly. In 2024, Marriage and Family Therapists (MFTs) and Mental Health Counselors (MHCs) were also permitted to bill Medicare directly.
What if a new mental health issue comes up with the patient?
The supervisor would need to be involved. Incident-to is only for follow-ups in the existing Medicare plan. If something new arises, the supervising provider is required to see the patient and update the plan prior to providing ongoing follow-up under incident-to.
Can ADHD medication management be billed under incident-to?
Yes. If a psychiatrist creates the plan and the nurse practitioner, or physician assistant, follows-up under incident-to, then it is acceptable. This is common incident-to service in mental health fields.
What if I bill incident-to incorrectly?
Medicare has the authority to deny claims, recoup payments, or audit your practice. In order to best protect yourself, keep good notes that indicate supervision.
What if a patient refuses to see the supervising provider?
You would not be able to bill incident-to if this occurs. The supervisor must see the patient to establish the care plan. If the patient won’t agree, bill under the clinician who provided the service if they are eligible to bill Medicare.
Is incident-to applicable for telehealth visits?
Yes, in some scenarios. If the service requires direct supervision, Medicare permits telehealth visits with live video until the end of 2025. If the service is under the general supervision rule, the supervising provider does not have to be present with the patient, and does not have to be on video either. The rest of incident-to rules still apply.